In an era where scientific advancements are pushing the boundaries of what is possible, the concept of human enhancement has become a topic of intense debate. With technologies such as CRISPR, being able to edit your own genetic makeup, the possibilities for enhancements are endless.

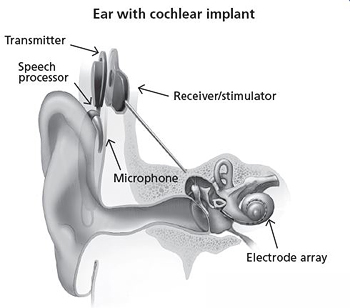
Human enhancement is the use of technological interventions to enhance human capabilities beyond what is ‘normal’. This includes physical, cognitive or sensory capabilities, enhancing the performance and well-being of patients.
In the past, prosthetics included wooden limbs with limited movement and comfort. The evolution of prosthetics has improved overtime and now with the development, integration of technology and artificial intelligence (AI), we are able to do what was only possible in science fiction.
A 46 year old male was able to regain movement in his arms with the use of AI. With plans already being made for chips to be implanted in our brains by Elon Musk, founder of neurotechnology company Neuralink, he quoted, “Initial users will be those who have lost the use of their limbs. Imagine if Stephen Hawking could communicate faster than a speed typist or auctioneer. That is the goal.” We are certainly not far from these developments.
These advancements hold the promise of improving the lifestyle and health of those effected, effectively changing their lives for the better. However it is important to think about the risks. Long term effects are currently unknown with no way of knowing until they are introduced it into society, but by then will it be too late to control. The risk of unintended consequences are always present.
Ethical implications:
Ethical questions are raised about the limits of intervention and the potential consequences for individuals and society. The notion of playing God, intervening in the natural order of things, contradicts many religious and philosophical perspectives. Moreover, informed consent are paramount as individuals must have the necessary information to make informed decisions about undergoing enhancement procedures.

Ethics and science need to shake hands - Richard Clarke Cabot
While some enhancements may address medical conditions and improve quality of life, others may be pursued for cosmetic or commercial reasons. This also raises concerns about fairness, equality, and access to these technologies. Who should have access to enhancement technologies, and at what cost? How do we define the limit?
Social & legal implications:
Human enhancement technologies could exacerbate social inequalities, widening the gap between those who can afford enhancements and those who cannot. Cultural attitudes toward enhancement, beauty standards, and even sports competitions may be profoundly influenced by these technologies. Regulatory frameworks must strike a delicate balance between fostering innovation and ensuring safety. Questions about marketing, prosecution for misuse of enhancement technologies, and setting legal limits on enhancement procedures add further complexity to the legal landscape.
Moreover, we may become a society increasingly dependent on technology to define human capabilities and identity. This challenges societal norms and values further, potentially reshaping perceptions of being human. Will we eventually lose our sense of what it really means to be a human?
Conclusion:

In conclusion, the ethics of human enhancement force us to confront profound questions about the nature of humanity, the limits of intervention, and the implications for individuals and society. While advancements in science and technology offer incredible opportunities for improving human capabilities, we must proceed with caution, mindful of the ethical, social, and legal ramifications. As we navigate this uncertain terrain, it is essential to engage in robust dialogue and ethical reflection to ensure that human enhancement technologies are used responsibly and ethically, for the betterment of all.




Very well written, with an excellent format and images. You’ve included interesting statistics and related it to personal ideas which…
This is a very well written blog, the format is as if you are talking directly to me. The ideas…
Love the Batman GIF :)
This is an excellent, well written blog. The narrative is engaging and easy to follow. It could be improved by…
This is a well-communicated blog. The it is written well with good use of multimedia. It could be improved with…