Hearing is a sense that I, and likely many others worldwide, take for granted. That said, around 1 in every 6 adults in the UK live with at least partial hearing loss. The technology behind cochlear implants piqued my interest after listening to the insights from users in the lecture, leading me to begin reading parts of Dr Yoder’s cochlear implant journey.
What is a Cochlear Implant?
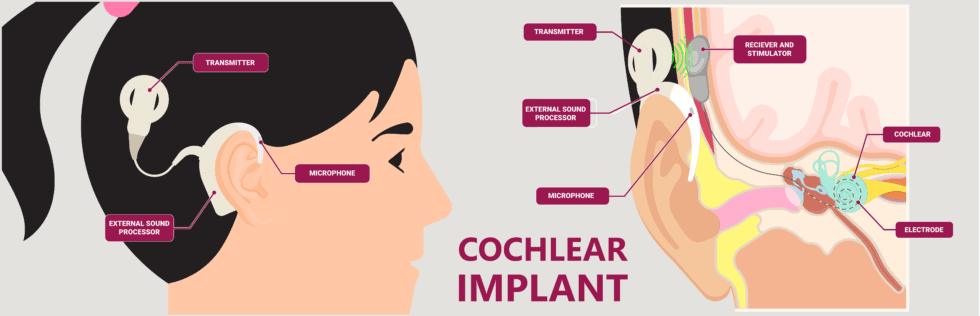
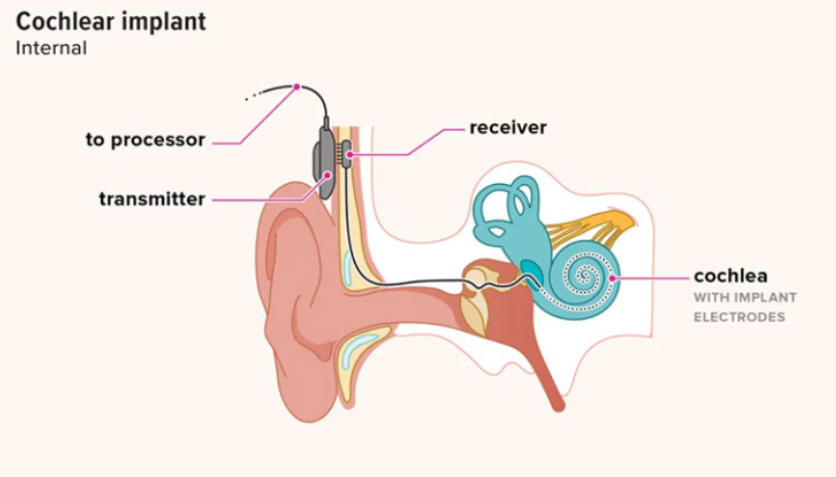
Cochlear implants are made up of both internal and external parts and require a relatively short surgery to fit. The external parts are made up of a microphone to pick up the sound waves, a language processor to convert the sound waves into electrical signals, and a transmitter to transfer these to the internal components. The language processor and microphone usually rest on the ear, while the transmitter is placed further back on the head. The transmitter is held on via a magnet fitted under the skin during surgery. This allows for the previously converted electrical signals to reach the string of electrodes inserted into the cochlear, which stimulates the auditory nerve directly.
Tuning
One aspect of cochlear implants that I found fascinating was tuning and the period over which it takes place; initial tuning usually takes place one month after the surgery, with periodic sessions after this to slowly ease users into the new sounds. This initially shocked me; “Why does this process take so long?”, I found myself thinking. However, after reading Dr Yoder’s experience with tuning as well as others (seen in the video below), I realised that hearing is not restored with the surgery, but with the practice users do to re-understand how everyday noises and speech sounds. The video below by Cochlear Americas documents four users and their experiences with training themselves to understand how to hear through their new implants, which I found very insightful.
Current and Future Research
A recent publication in Ear and Hearing in 2023 discussed advancements in tuning of cochlear implants, and how artificial intelligence can be used to outperform traditional tuning methods. The traditional method, despite performing less effectively, was preferred by participants, owing to it feeling more comfortable for them. I believe that this aspect of optimising implants should not be neglected; how the users think or feel about such methods, be it tuning or any other aspect of the implants, is of utmost importance.
A less recent article from the engineering department in Cambridge highlights how 3D printing can be utilised to improve cochlear implants. The fluids inside the cochlear ducts are highly conductive to electrical signals and implant users often, due to this conductivity, experience distorted sounds through their implants; this is known as current spread. The use of 3D-printed cochleae, paired with machine learning, allowed researchers to analyse and predict how current spread was impacted by the cochlea’s shape and conductivity. Dr Shery Huang, an associate professor in Bioengineering at Cambridge, suggested that this is an extremely useful application of 3D printing since data regarding patients must be kept private; Dr Huang was quoted in the article, stating that to solve this, “3D printing is a powerful tool to create physical models which might provide a well-characterised training dataset as a purpose-built surrogate to clinical data for machine learning”.





Very well written, with an excellent format and images. You’ve included interesting statistics and related it to personal ideas which…
This is a very well written blog, the format is as if you are talking directly to me. The ideas…
Love the Batman GIF :)
This is an excellent, well written blog. The narrative is engaging and easy to follow. It could be improved by…
This is a well-communicated blog. The it is written well with good use of multimedia. It could be improved with…