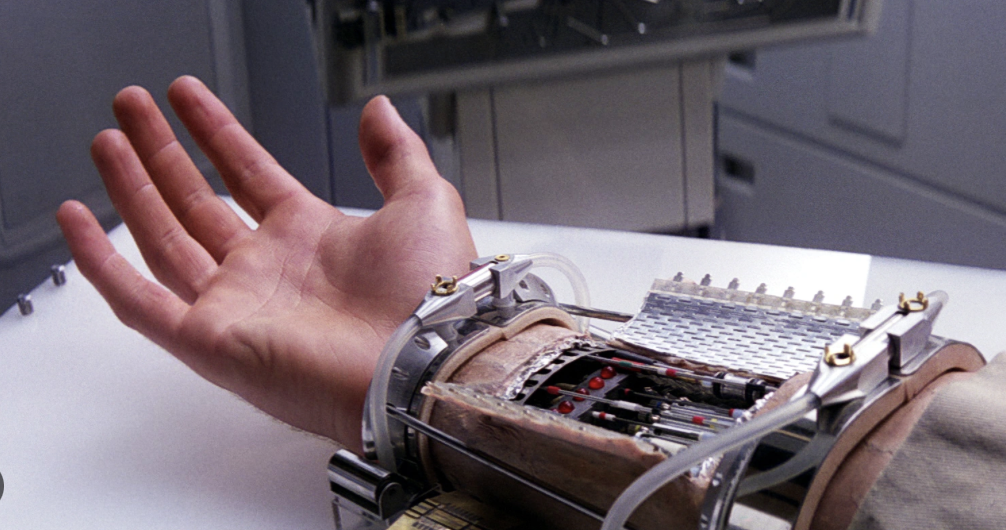
In the realm of fiction, prosthetics often take center stage, portraying characters who transcend physical limitations with cutting-edge technology. From Luke Skywalker’s robotic hand to Iron Man’s sleek armor, prosthetics in popular culture captivate audiences with their seemingly limitless capabilities. But how accurate are these portrayals when compared to the advancements in real-world prosthetics?

While the prosthetics depicted in fiction may appear futuristic and awe-inspiring, the truth is that they often stretch the boundaries of scientific feasibility. However, that’s not to say that there aren’t elements of truth behind these imaginative creations. Many fictional prosthetics are inspired by real-world advancements in prosthetic technology.
One area where fiction tends to diverge from reality is in the speed and ease with which characters adapt to their prosthetics. In many stories, characters seamlessly transition from being disabled to mastering their new limbs or devices in a matter of moments. In reality, the process of adjusting to a prosthetic limb can be long and challenging, requiring extensive physical therapy and training to regain functionality. The Portsmouth Regional Prosthetic Service outline a 5 Stage Rehabilitation Process and they state it usually takes 3-6 months to adjust using the prosthetic limb, such as a leg, through intensive physiotherapy.
Moreover, while fictional prosthetics often boast superhuman abilities, such as enhanced strength or agility, real-world prosthetics are still limited by the constraints of current technology. While significant advancements have been made in creating prosthetic limbs that mimic natural movement, they are still a far cry from the fantastical capabilities seen in movies and television shows.
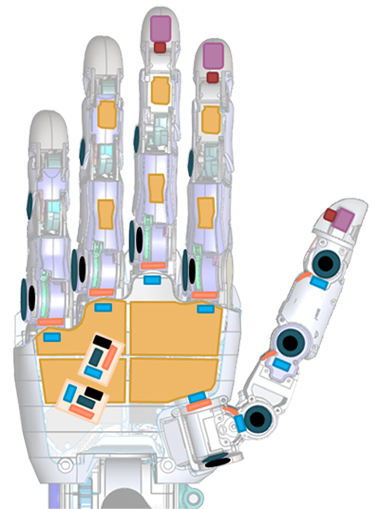
However, that’s not to say that real-world prosthetics aren’t impressive in their own right. In recent years, advancements in materials science, robotics, and neuroscience have led to significant improvements in prosthetic technology. For example, prosthetic limbs equipped with myoelectric sensors can detect electrical signals from remaining muscles, allowing users to control their prosthetics with astonishing precision. Studies have shown promising clinical outcomes for patients after transhumeral amputation, who received a neuromusculoskeletal prosthesis that allowed intuitive and unsupervised daily use over several years.
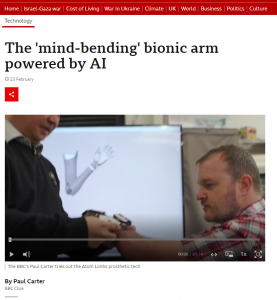
Additionally, ongoing research in the field of brain-computer interfaces (BCIs) holds promise for the future of prosthetics. BCIs allow users to control prosthetic limbs directly with their thoughts, bypassing the need for muscle signals altogether. While this technology is still in its infancy, early experiments have shown promising results and could eventually lead to prosthetics that are even more intuitive and responsive.
In conclusion, while the prosthetics depicted in fiction may push the boundaries of scientific reality, they are often inspired by the advancements and possibilities within the field of prosthetic technology. While we may not yet have prosthetics with the capabilities of those seen in movies and TV shows, real-world prosthetics continue to evolve and improve, offering hope and opportunities for individuals with limb differences to lead fulfilling and active lives. As technology continues to advance, the line between fiction and reality may blur even further, bringing us closer to the futuristic visions of prosthetics seen on screen.
Sources:
Ortiz-Catalan, M., Mastinu, E., Sassu, P., Aszmann, O., & Brånemark, R. (2020). Self-Contained Neuromusculoskeletal Arm Prostheses. New England Journal of Medicine, 382(18), 1732–1738. https://doi.org/10.1056/NEJMoa1917537










Very well written, with an excellent format and images. You’ve included interesting statistics and related it to personal ideas which…
This is a very well written blog, the format is as if you are talking directly to me. The ideas…
Love the Batman GIF :)
This is an excellent, well written blog. The narrative is engaging and easy to follow. It could be improved by…
This is a well-communicated blog. The it is written well with good use of multimedia. It could be improved with…