
Following our lecture on prosthetics and orthotics, I became interested in the affordability of the new prosthetic technology in the UK and in developing countries. From the age of nine to sixteen I was a competitive swimmer, this lecture reminded me of a girl I swam with who had a below the knee amputation, she always struggled with her prosthetic limbs and swimming. This was mainly due to one factor; she could not afford the newest technology and the NHS would only cover certain costs.
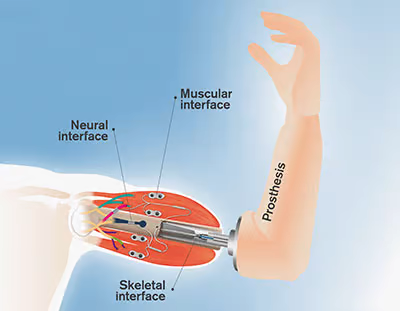
What is a prosthetic limb?

An artificial substitute for a missing part, such as an eye, limb, or tooth, used for functional or cosmetic reasons
medical dictionary
This prosthetic toe has been dated between 950 – 710 BC. It was composed of wood and leather
Prosthesis technology has been around since 950 BC, prosthetic limbs are used after a limb or body part can no longer be used due to incidents such as disease, trauma, or a medical condition present at birth.
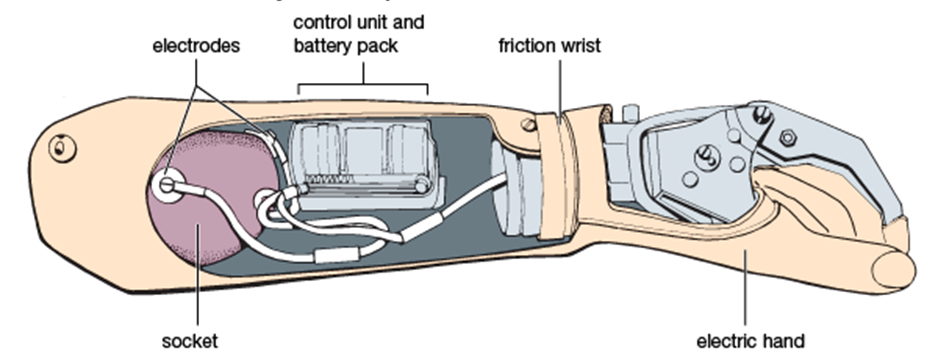
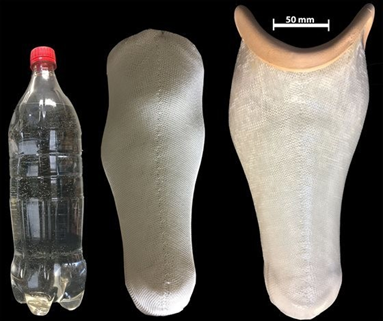
In recent years prosthetics are made from advanced plastic and carbon fibre. The leaps in our technology astounded me, but it left me thinking with increasing technology there must be an increase in price. After investigation I found that the NHS is improving significantly when it comes to accessibility and in November 2022 the new bionic arm became available through free healthcare this came as a shock as I previously had other ideas regarding the accessibility in the UK.
As I read around the subject further, I found that I was more interested in prosthetic limbs in developing countries especially after learning that the professor delivering our lectures on prosthetics is running an accessibility campaign.
Approximately 40 million people have a need for a prosthetic leg in the developing world yet a mere 5% have prosthetic options. The newest technologies are expensive; I was astounded when I realised many people don’t have access to the most basic prosthetics! The citizens that have access may not even be able to afford the prosthetic limb available. I have come across an organisation called LIMBS they aim to develop new designs to allow people in developing countries to have access to prosthetics. They focus on rehabilitation processes amputees can go through which supports amputees mentally and physically. They call for social change to allow these countries to work through their emotional trauma whilst also providing high-quality, low-cost prosthetic limbs.

The LIMBS project is under the borgen project, which is a non-profit organisation. This provides a good source of information when researching prosthetics in developing countries and the real-life effects of their work.
Click on the picture to find out more.
What is Southampton university doing to help?
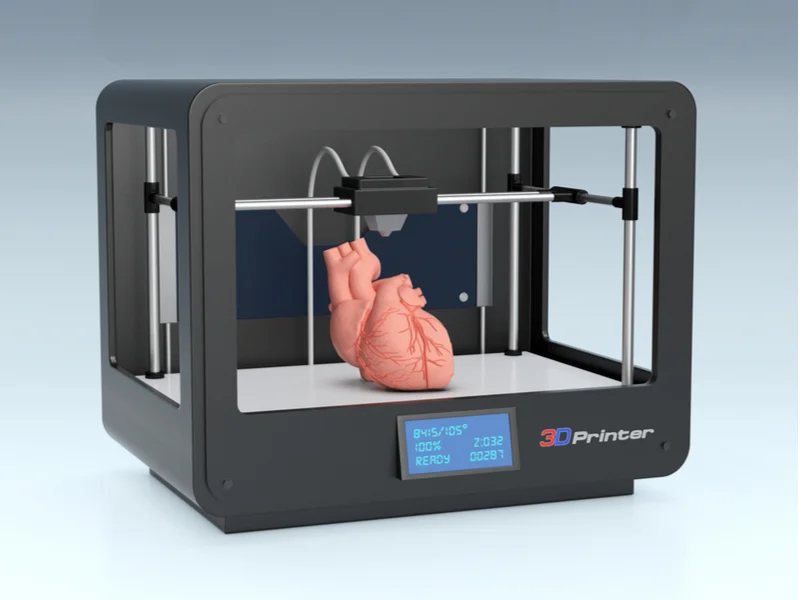
Dr Alex Dickinson is currently leading a multidisciplinary team of health scientists and engineers to discover how we can use technology to help improve accessibility to prosthetic limbs in Cambodia. They are looking at the growing number of amputees and the countries inability to keep up with the high demand. They have been researching into portable 3D Scanners and most importantly Dr Maggie Donavan-hall has been looking at what technologies will realistically meet their needs, culturally and socially. The key aspects I took away from reading about this research is the need to tailor prosthetics and orthotics to the country and the people, the prosthetics need to work well with what is already in place in that country. As well as this it made me think about how else portable and personalised prosthetics having would help communities. For example, it was explained that it would also help due to decreasing waiting times to see a clinician, the clinicians would be mobile meaning they can take these devices to the patients. This allows the patients to take less time off work. I think this is a big step as it means more members of the community can come forward to receive help as they won’t be scared about it affecting their jobs.
https://www.southampton.ac.uk/news/2019/01/a-step-change-in-prosthetics.page: Prosthetics in developing countries




:focal(808x298:809x299)/https://tf-cmsv2-smithsonianmag-media.s3.amazonaws.com/filer/53/c3/53c3b6a3-929b-43f1-bf61-2d2cafbbecca/lacks1.jpeg)






{kind=link}
This is an initially reflective and well researched blog showing how you have chosen to explore the emerging field of…
This is a good attempt at a blog, where you reflect on your recent learning at a lecture/workshop to describe…
This is a fair to good blog, reflecting on your recent learning in some of your modules. You provide a…
This is an engagingly written and reflective blog focussed in general on ethics in medicine. You might improve by citing…
This is a good and well written an presented blog on an original subject - biofilms on implants. You explain…