From internal procedures like knee or hip joint replacements, to external ones like replacement limbs, prosthetics allow hundreds of thousands of people each year increased quality of life and mobility. As someone with a background in animal ecology, I became interested in how prosthetics for animals might be created; they have very different morphology and requirements to humans, with stronger forces being exerted on them, and the animal’s natural behaviour needs to be considered.
One example of prosthetics being used for non-human patients is, of course, Prof. Noel Fitzpatrick, who treats pets around the UK, for example Oscar, a cat who lost his hind limbs, and had them replaced with Intraosseous Transcutaneous Amputation Prosthetics (ITAP), where holes are drilled into the residual limb’s bone and the implants are then attached, allowing the skin to bond to the prosthetic, creating ‘pegs’ onto which the limb itself can then be attached following a recovery period. Similar methods for bone-anchored limb prosthetics are being considered for humans, though still in its early stages. Even a recent study performed on 16 cats and 4 pigs finds issues with infection at the stoma, and a high failure rate of integration. Regardless, it is true that prosthetic techniques being developed in the field of veterinary science can have implications for human medicine.
Figure 1 (Supervet, 2009) – Oscar the cat with his Osseointegrated hind limbs. Note the interaction between the patient’s skin and the limb.
But what I was most interested in was wild animals, whose requirements would be a lot different to pets’. That’s how I ran into Winter, a bottlenose dolphin whose tail was lost in a crab trap in 2005. Over a year and a half later, with a lot of work from a dedicated team, a prosthetic tail was completed and fitted onto Winter. Unlike an arm or a leg, a tail can’t simply stay solid as the animal moves, but must move along with it, hold its position under water and under the force of a large animal using it to propel its movement, not cause further injuries to Winter, and, of course, perform its function as a tail. The resulting material created from this research, WintersGel, can now be used for human patients, especially athletes as it is softer and distributes weight more evenly than other liners, reducing pain and pressure exerted by the limb.
Video of Winter’s tail prosthesis being fitted, showing some of the process of adapting to he new limb
There are many other cases of prosthetics being used in wildlife, from an injured Bald Eagle with a prosthetic beak, to a young elephant with a prosthetic foot, to a 3D-printed leg for a Secretary Bird at a bird park who injured her leg, and, prevented from engaging in her natural behaviours, began engaging in behaviour associated with poor welfare. There has even been a tiger in east Germany who, experiencing pain from arthritis, had a hip replacement, although a more recent operation hasn’t been as successful, and the tiger who underwent it had complications. This, as well as other cases where operation may have had more negative than positive consequences for the animal, raise the importance of ethical considerations in wildlife prostheses. Are these operations always necessary? Do they increase the animal’s quality of life, or do they add unnecessary stress to an animal’s life who might not survive for very much longer, or who, unable to engage in their full behavioural repertoire, might exhibit stereotypies or other negative behaviours? With humans, we can operate on the basis that each of us should have autonomy over what happens to our own bodies, and that informed consent is crucial in these and other procedures, but who should get to decide when the patient can neither understand what is happening nor communicate their preferences on the matter?
Recently I have been reviewing and watching content regarding our rapid advancements in technology which has given us the ability to replace body parts with prosthetics or other artificial devices. However, with this ability a significant ethical question arises of whether it is ethical to enhance our bodies beyond their natural capabilities. I drew inspiration for this post from the video by the Pew Research Centre included at the end.
One of the key ethical concerns surrounding replacement body parts is the question of what it means to be human. Humans have historically viewed themselves as distinct from other animals because of our unique combination of physical, emotional, and intellectual capacities. The introduction of artificial enhancements to our bodies could blur the lines of what it means to be human, and could even lead to the creation of new, non-human species. This raises important questions about how we define humanity, and what the implications of altering our bodies could be for our identity as humans.
Another ethical issue that arises with replacement body parts is the potential for inequality. While the technology for artificial replacements has become more accessible in recent years, it still remains out of reach for many people, particularly those in less developed countries or who do not have access to proper healthcare. If only a select few individuals are able to afford or access these enhancements, it could lead to a new form of inequality where those who can enhance their bodies are more advantaged than those who cannot.
There is also the concern that replacement body parts could become a form of social pressure. If certain enhancements become popular or even necessary to keep up with societal norms, it could create an environment where people feel pressured to modify their bodies even if they do not want to. This could lead to a lack of individual autonomy and could even be seen as a form of discrimination against those who choose not to enhance their bodies.
However, there are also arguments in favour of replacement body parts and enhancing our bodies. One of the primary benefits is the ability to improve the quality of life for individuals who have experienced physical limitations due to injury or illness. By replacing a lost limb or enhancing an impaired sense, individuals can regain their independence and improve their overall well-being.
Archive Photos//Getty Images
Additionally, the development of replacement body parts has the potential to drive medical innovation forward. The same technology used to create prosthetics and artificial enhancements could also be used to develop new treatments for a variety of medical conditions however it would inevitably also be used military purposes as well.
To summarise the ethics of replacement body parts and the idea of enhancing our bodies is a complex issue with no easy answers. While there are certainly concerns about the potential implications of modifying our bodies, there are also clear benefits to individuals and society as a whole. As we continue to advance in technology and medical innovation, it will be important to carefully consider the ethical implications of these advancements and to work towards a future where everyone has access to these life-changing technologies.
From the lectures on tissue engineering, I found the idea of fixing the body with the same materials that make up the body really interesting, and how this can help with rejection which is faced by foreign materials in the body. This led me to look more into recent advances in tissue engineering, where I came across this news article about a new biomaterial with the potential for healing damaged heart tissue after a heart attack.
What is it?
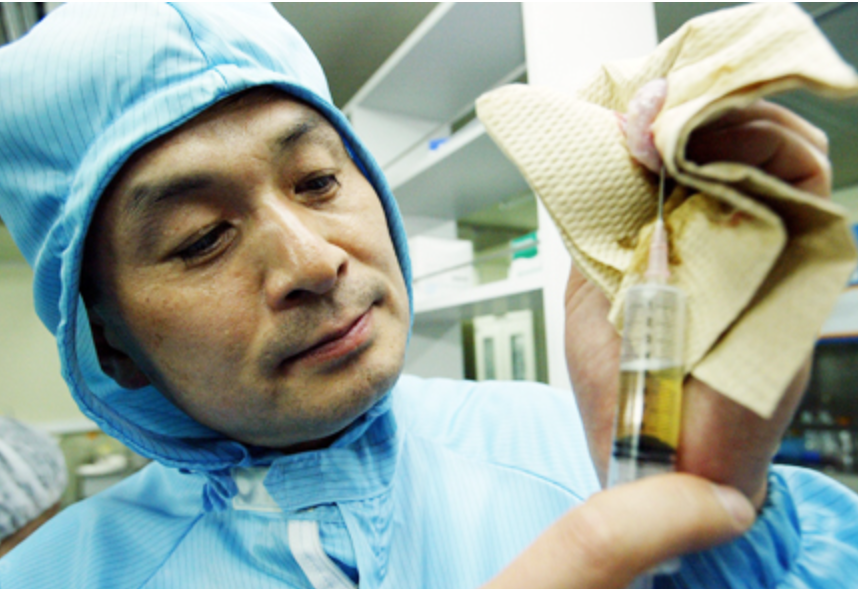
A team at the University of California San Diego has developed a new hydrogel, which is a polymer chain complex that can hold a lot of water. The hydrogel contains extracellular matrix (ECM), from the myocardium, or heart muscles. The ECM has been decellularized to isolate the matrix, enzymatically digested, and fractionated. In the body, cells exist inside a matrix, which contains proteins and other molecules to give structure to tissues and aid in cell communication. The original hydrogel that was developed was too large to target leaky blood vessels. This issue was solved by centrifuging the gel in its liquid stage to remove larger particles.
A hydrogel being made.
How does it work?
The hydrogel is injected intravenously, taking advantage of the bloodstream to access hard to reach organs. After a heart attack, gaps form between the endothelial cells which line blood vessels. When the hydrogel reaches the damaged tissue, it binds to these cells, bridging these gaps and promoting new cell growth and repair, and also reducing inflammation. The gel takes roughly 3 days to degrade after administration.
In their initial clinical trial, the gel was directly injected into the heart muscle. This came with the disadvantage of having to wait at least a week after the heart attack, as injecting the damaged tissue by needle directly after is likely to do more harm than good. Intravenous injection can be done immediately. The hydrogel can then work together with other treatments such as angioplasty or a stent. In addition, the gel is more evenly distributed around the tissue rather than being concentrated around the site of injection.
The Next Steps
This new way of administering the gel has been successfully tested on rodents and pigs to treat damaged heart tissue. The research group are looking to get authorisation from the FDA to perform human trials, with plans to start in the next couple of years. They are also exploring the potential of the hydrogel to treat other inflammatory diseases such as traumatic brain injury and pulmonary arterial hypertension with preclinical trials on rodents.
In the UK there are around 100,000 hospital admissions every year for heart attacks- or one every five minutes. Over the past 50 years, there has been major advances in treatment and survival. In the 19080s roughly 25% of people having a heart attack would die, nowadays, if treated quickly, the chance of dying during a heart attack is 2-4%. In the future this number will hopefully reduce even more with advances in bioengineering.
References
British Heart Foundation, 2023. UK Factsheet. [Online] [Accessed 9 March 2023].
Spang, M. T. et al., 2022. Intravascularly infused extracellular matrix as a biomaterial for targeting and treating inflamed tissues. Nature Biomedical Engineering, 29 December, Volume 7, pp. 94-109.
Thomas, M., n.d. Focus on: Heart Attacks [Interview] n.d.
University of California – San Diego, 2023. Groundbreaking Biomaterial Heals Tissues From the Inside Out. [Online] Available at: https://scitechdaily.com/groundbreaking-biomaterial-heals-tissues-from-the-inside-out/ [Accessed 8 March 2023].
Recently my family received the unfortunate news that my grandmother has been diagnosed with stage 1 Parkinson’s disease. This came as a shock to me and since then I have been trying to educate myself about this condition and figure out the best way to support her.
Parkinson’s disease (PD) is a progressive neurological disorder affecting more than 10 million people worldwide. This is caused by the degeneration of dopamine-producing cells in a region of the brain called the substantia nigra leading to a decrease in the dopamine neurotransmitter that is essential for controlling movement and coordination. This decrease in dopamine leads to motor symptoms including hand tremors, slow movement, limb rigidity, imbalance, and non-motor symptoms including cognitive impairment, mental health disorders, sleep disorders, and so on.
What causes this degenerative condition?…we don’t know!
The underlying mechanisms responsible for the deterioration of nerve cells associated with PD are not yet fully understood. Researchers believe a combination of genetic and environmental factors cause the dopamine-producing cells to die. Some of the factors that have been linked to PD include aging, exposure to certain toxins, head injuries, and genetic mutations (Parkin and PINK1 gene).
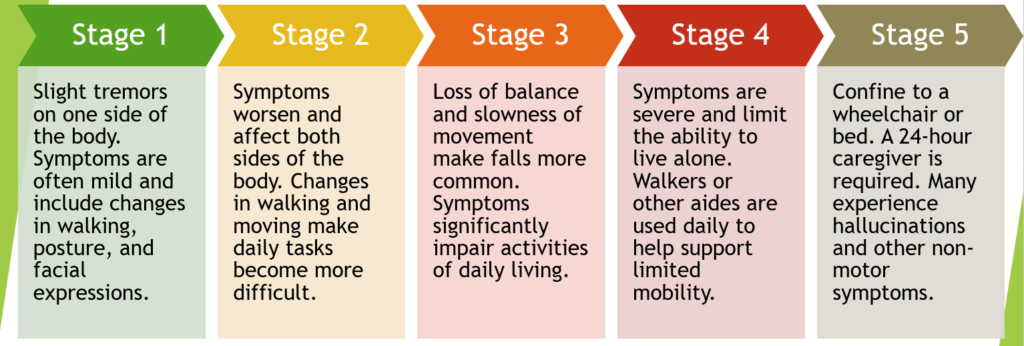
5 stages of Parkinson’s disease
PD can start with mild symptoms and go unnoticed, but as the condition worsens, symptoms become more obvious and can have a big impact on daily life.
Treatments, not cures: Living with Parkinson’s disease
Medications: Drugs such as levodopa, dopamine agonists, MAO-B inhibitors, and COMT inhibitors can help manage the motor symptoms of PD.
Physical therapy: Regular exercise can help improve motor function, muscle strength, increase flexibility, and reduce stiffness, which can be very important in the early stages of the disease.
Deep brain stimulation: This procedure involves implanting a device called a neurostimulator which sends electrical impulses to specific parts of the brain to lessen the symptoms of PD.
My grandmother’s doctor has prescribed medication to help manage her symptoms and advised her to stay active in any way she can. Is this enough? PD usually develops in people over 60 but it can also occur in younger people, what about them? Is this the only solution?
Unsatisfied with this information, I continued researching until I came across a useful article that offered fresh new perspectives; Stem cells: Parkinson’s treatment breakthrough. Preclinical studies using mesenchymal stem cells have shown promising results for treating PD; aiming to reduce neuroinflammation, modulate the immune system to prevent disease progression, and repair or even replace, the damaged or lost, dopamine-producing cells in the brain. This could lead to significant improvements in motor symptoms like tremors, stiffness, rigidity, and difficulty with movement.
While more research is required to confirm the effectiveness of stem cell therapy on PD, this gives me hope for the future. Stem cells are so powerful, they can renew themselves indefinitely, and be manipulated in the lab to develop into specific cell types, possessing a tremendous potential to be used in therapies to treat a variety of diseases and conditions, why not PD be one of them?
I have recently had the opportunity to meet a very successful surgeon who specialises in Hip replacement and trauma surgery. Prof. Douglas Dunlop was kind enough to invite me to his clinic where a one hour conversation inspired me to write this blog. He gave me a lot of insight about hip replacement surgery and with that, exactly what could go wrong.
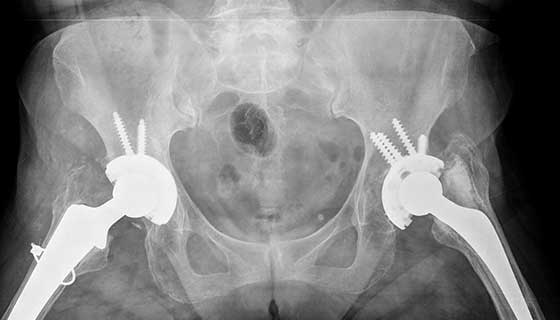
Initially Prof. Dunlop showed me a couple images of hip replacement x-rays, such as the exemplar. One in particular was an image of an anonymous patient, an elderly male who had undergone multiple hip replacement surgeries. Prof. Dunlop and I have discussed why more than one surgery was needed, which leads me to talk about Hip replacement, and it’s potential risks. It might be miss-leading for me to use that title considering it’s impossible to write about every setback, but I will aim to discuss the ones I have learned about.
Going back to the patient. Initially the male had a 3M Capital hip, which due to poor performance lead to revision. Prof. Dunlop explained that the femoral head of the implant became loose in the joint along with the cement holding it together. The friction exerted on the socket lead to osteolysis and screws were needed to keep the implant in the shallow socket. I will not be going into a lot of detail on the 3M Capital hip, but upon further research I have stumbled upon a risk assessment document. It pinpointed that revision was more common in males, and the findings from the report were conclusive; the 3M Capital hips had higher revision rates than other commonly used prosthesis. In addition, with each round of surgery, the hip stem needed to get larger. To make room for a new implant, the femur needs to be reamed. This in turn sacrificed the bone, increasing the risk of fracture, along with loosening of the prosthesis or infection.
Why do hips fail?
I was surprised to hear that the patient had over 3 hip replacement surgeries. On that note its very important to not only think about the failure of the prosthesis, but also why they are initially needed.
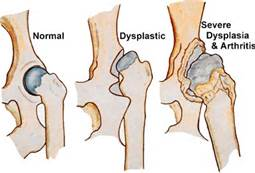
In our discussion, Prof. Dunlop identified the two most common causes of surgery in his patients; arthritis and hip dysplasia.
Hip dysplasia is a medical condition where the hip socket does not fully cover the femoral head. This in turn creates a very shallow socket, which is very susceptible to osteolysis. Friction damages the labrum that lines the joint and can lead to hip labral tear, causing pain and discomfort. Arthritis gives rise to similar symptoms and can have multiple causes.
(MORE) problems with prosthetics.
Wear and tear has a honorary mention on this blog. It seems to be one of the leading culprits for hip surgery, damaging not only the bone, but the implant itself. Below is a list of a couple other things that could go wrong:
Loosening – causes pain and can lead to an inflammatory response
Dislocation of the prosthetic
Tendonitis – inflammation and injury of tendons
Fractures – example of stiffer hips made of cobalt chrome with 3.4% fracture rate and CPT (Zimmer brand) previously used at Southampton General with a high fracture rate.
Prof. Dunlop also highlighted that often a ceramic head is used in combination with a metal stem for the prosthetic. Many surgeons are now moving away from monoblock prosthetics as the acetabular component cannot be changed.
Where to go from there?
Hip prosthesis may lead to a lot of uncertainty, but just like any other invasive procedure it comes with risks and benefits. I once met a lovely woman called Anne; she has had both her knees and one hip replaced, and yet she has no complaints. In fact she said that the surgery was “life changing”. It allowed her to carry out day to day activities at the age of 87!
Despite ‘all that could go wrong’, it is very important not to overshadow all the benefits that come with prosthesis. The risks can be analysed, prompting researchers and surgeons to develop more successful treatment options and prosthetic joints with less complications. It is fascinating to see what the future of prosthesis may hold!
A large review study demonstrated that hip replacements last 25 years in approximately only 58% of patients.
Cloning is a phenomenon that scientists use to make exact copies of living cells and genes. Dolly the sheep was a breakthrough where scientists had cloned an entire sheep using the complete genome of another animal adult. As miraculous as this may seem, there is an everlasting debate regarding the ethics of this technique. Questions rise as to whether cloning will ever been seen as right or wrong.
Why was I fascinated by this topic?
During a workshop today I came across a case study about a stem cell scientist, Woo Suk Hwang, who sparked my interest towards the debate on ethics, claimed to have utilised eggs from ‘paid donors and junior members of his team’ after a long time denying this very fact. At the time of Hwang’s research, paying donors for their eggs was not illegal in Korea but he was put in a position of jeopardy due to his ‘ethical and unlawful’ actions.
This raises a question of ethics as to whether it was fair for Hwang to be penalised for performing such invasive procedures on paid donors, or whether due to their being no law against it should mean that Hwang should not have to be punished.
I found this interesting as there is a very broad spectrum as to what one may find right and what they may find wrong, and often we are left in a grey area of neither or. It could be argued that the procedure was unethical as an incentive behind a donation makes you question whether the women was donating her egg because she wanted to or had to. For example, it could also be seen as an easy fix out of poverty which leads onto the argument whether one with a ‘supposed to have moral high ground’ should be performing a procedure on such donors.
On the flip side, Hwang did not do something that was against the law at the time and I could argue that if incentives had not been put in place, we would have less donations and more people would suffer as they would not be able to get any treatment as there would be a lack of it.
Will there ever be an end?
It made me question whether such a case would ever come to a conclusion to whether his actions were right or wrong. Would there have to be an international law put into place for the whole world to follow? And even so, the law differentiates from ethics and many different cultures have different stances and viewpoints. In Hwang’s case, a researcher had donated her organs as she had made a mistake during the experiment setting them back months, and due to this she felt obligated to ‘ make right of a mistake’ which is a collectivist and patriotic way of thinking, which was common in South Korea. Other cultures may be more lenient with their mindset when making mistakes.
Ethics will always be a topic for debate and there will always be two opposing opinions as with Hwang’s’ case I could argue both cases and personally still be torn whether he was right or wrong. In conclusion, it may just all come down to what opinion / viewpoint is the lesser of two evils?
Upon starting my Engineering Replacement Body Parts module, the prosthetics joints and limbs lectures sparked a particular interest. It became evident to me that when an individual loses a fully functioning body part, alongside the obvious physical loss, there is also an element of mental loss in their sense of being. There becomes an immense divide between being ‘disabled’ and ‘able’.
Over half of the world’s population suffers from some form of cognitive, motor or sensory disease, and at what expense? The lack of efficient technology?
So… What if there was a way to enhance people’s capabilities beyond their losses, restore motor function and finally bridge that gap between limitation and potential? Luckily enough, we live in a period of time where there CAN be a way. A way we now call bionics.
Bionics is defined to be:
‘The science of creating artificial systems or devices that can work as parts of living organisms’
By making it possible to replace whole organs to mimic that of the real ones, whether it be your eyes, ears, legs or even your brain, we are now able to massively improve the quality of life of those who have lost limbs, so they can freely go about day-to-day life like they once did before.
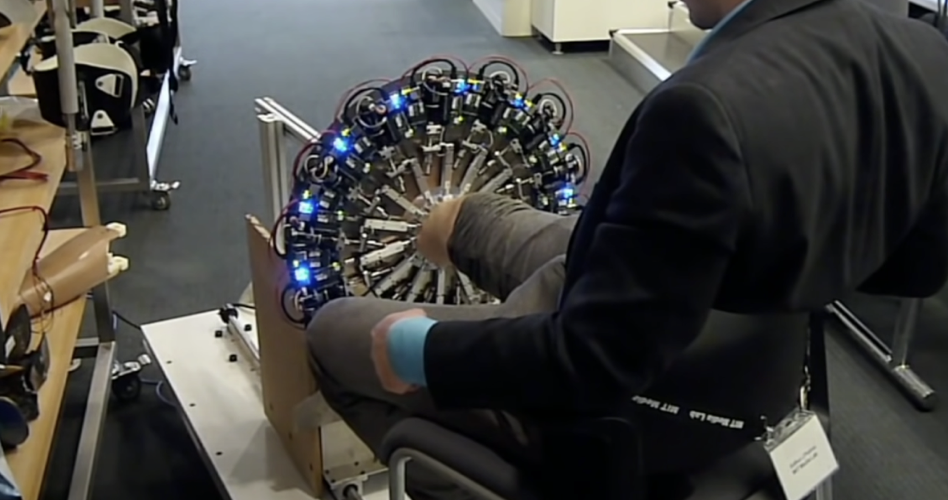
Bionic Integration with Hugh Herr
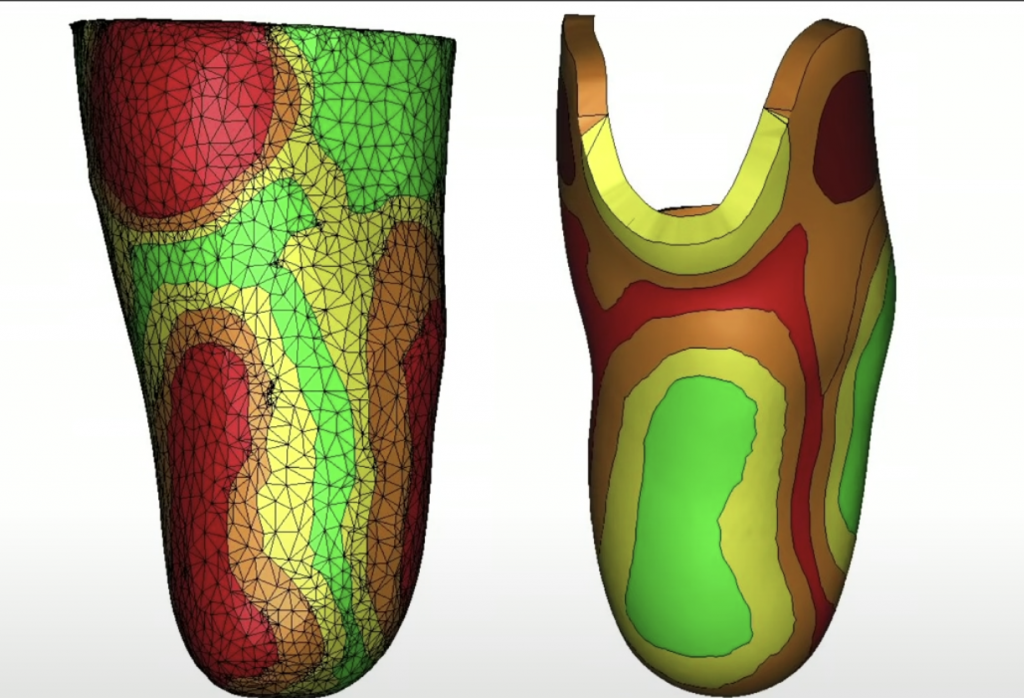
In an incredibly moving TedTalk in 2014, Hugh Herr explains how bionics shaped his life. After losing both of his legs in a climbing accident in 1982, technological innovation allowed Herr to cure his own disability with optimal support, and in doing so, discovered the beauty of the flexibility in the artificial part of his body.
Through mathematical models, imagining and robotic tools, his bionic limbs were able to attach to his true body through synthetic skins with stiffness variations mirroring his underlying tissue biomechanics. To add to that, through bionic propulsion allowed the bionic limb to emulate normal muscle function, or even at an advanced level. This was critical for Herr and his athletic ability. To add even further, electrodes measuring electrical pulse of muscles communicated to bionic limb so if he thinks about moving, he moves!
He took advantage of this flexibility and returned to climbing, eliminating his disability. Herr, as the head of the MIT Media Lab’s, is now building the next generation of bionic limbs and robot prosthetic that resemble biological materials.
The moral of the story is, despite losing both of his legs, the importance of bionics and the characteristic ability to use electromechanics attached to the body and implant them inside the body meant that Herr’s quality of life only flourished. He did not let it diminish him, nor destroy his self-wholeness. This should be the hope for all those who suffer from a similar story.
What do the ongoing advancements in ‘Bionics’ mean for the future of ‘disability’?
In decades to come, if the progress continues, we could see a world free of disability. Where a hand could have additional functional fingers, or an eye could improve low light vision and zoom in to make faraway objects clearer, or the paralysed can walk primarily based on artificial neural networks and swarm intelligence.
While artificial limbs are not nearly as good as a natural one, someday, we might advance to the point where artificial limbs might become superior to natural ones, available to everyone that needs it.
That being said, even those with normal physiology have appeared to use exoskeletal structures following the same principles to augment things like human walking, running, climbing etc. In doing so, it reduces metabolite cost and suggests that we are going into a time where these designs can make us stronger, faster and more efficient
To conclude…
Every being on this earth deserves a right to a life free of disability and full of ability at basic physiological function. The ongoing advancements of bionic technology show that as a human race, we are dependent on its growth to optimise our living. So perhaps humans cannot be disabled, but technology?
I have always had an interest in the ethics behind scientific research, in particular the discussions around using human tissues in research. However, the case study of the Alder Hey Organs Scandal was mentioned in the law and ethics lecture and I had never heard of anything like it. It certainly piqued my interest as retaining children’s organs without consent or permission seemed such a baffling concept to me.
An ethical minefield
A scene from the film adaptation of “Never Let Me Go” where one of the now grown-up children is completing one of his “donations” (https://musingsaboutfilm.wordpress.com/2015/05/20/2-ethical-issues-in-never-let-me-go/)
Alder Hey is an NHS hospital in Liverpool that was the centre of a scandal when in 1999 it came to light that during post-mortem investigations of children between 1988 and 19951, the pathologists were retaining the organs of the deceased children without the knowledge or consent of their parents2. This blatant “harvesting” of organs reminded me of a book I read recently entitled “Never Let Me Go” by Kazuo Ishiguro. To summarise, the book is the story of 3 children who grow up and realise they are clones of members of the public, and their role is to “donate” their organs until they eventually pass away. I found the dystopian science fiction nature of the book incredibly fascinating, and it shocked me how events that are eerily similar to those in the book have actually happened in most people’s lifetimes.
Why were the organs retained?
After the lecture I wanted to find out more about how activities that could well be described as “dystopian” managed to occur, bypassing the consciences of those involved. I initially assumed that the organs had been used for donations to children that needed transplants, but after thinking more about it whilst doing my research I realised that the organs would not be of use by the time the post-mortem occurred. Then why were the organs taken? Upon reading some journal articles from the years following the scandal I found out that many of the organs were not histologically examined, or used for educational and research purposes.
The headlines in some national newspapers following the scandal (https://www.cell.com/current-biology/pdf/S0960-9822%2801%2900078-1.pdf)
The reason the organs were retained (even for no apparent purpose) lies in the vague wording of the Human Tissue Act 1961 in which pathologists could retain tissues if there was a lack of objection, rather than informed consent. Therefore, by not informing the parents of the children about the reality of post-mortem procedures, there was a lack of objection and thus the ability to retain the tissues1. However, this cannot justify the utter devastation experienced by the parents of these children, who already had experienced the awful loss of a child, as they came to the realisation that their child had been incompletely buried.
Additionally, I researched more about Dr Van Velzen, who was mentioned in many of the papers I read. I discovered that he was a pathologist who was struck off the General Medical Council for storing over 1000 organs from 850 children in jars in a dirty cellar as they slowly decomposed3. This is a particularly uncomfortable revelation as it is practically impossible to justify the decisions made by Dr Van Velzen.
Moving forwards
I found researching this case further incredibly insightful because I was unaware of anything like this happening in the recent past, and there was so much to find out. Cases like the Alder Hey Scandal have a huge importance in future scientific ethics discussions to ensure history does not repeat itself. The scandal led to the Human Tissue Act 2004, which clearly outlines the need for explicit consent for retention of tissues for research or other reasons.
The memorial stone commemorating the children whose organs were retained (https://en.wikipedia.org/wiki/Alder_Hey_organs_scandal)
Reference List:
Burton, J. L and Wells, M., (2002). The Alder Hey affair. In: Archives of Disease in Childhood (86/1). London: BMJ. pp. 4-7. DOI: https://doi.org/10.1136/adc.86.1.4
Bauchner, H. and Vinci, R., (2001). What have we learnt form the Alder Hey affair? In: British Medical Journal (322/7282). London: BMJ. pp. 309-310. DOI: https://doi.org/10.1136%2Fbmj.322.7282.309
Dyer, O., (2005). Alder Hey pathologist is struck off medical register. In: British Medical Journal (330/7506). London: BMJ. p. 1464. DOI: https://doi.org/10.1136%2Fbmj.330.7506.1464-a
Before I begin this blog on philosophical arguments and medical consents, it should be noted that there usually is no “real” definitive ethical answer to an argument as I follow JS Mill’s view that knowledge is not infallible, and that All sides contain plausible explanations. Truth, lies, or partially true, should be brought together in discussion (JS Mill, On Liberty).
Case analysis
In the paper by Murray (1990), the author stated many legal cases through out the history, providing evidence in how the medical consent was progressed. From the legal cases provided, in general, it can be observed that utilitarianism and deontology were combined. Although mainly, in the cases where informed consent was present, patient-centred deontological view is followed, and that the surgeons will respect patients’ individual liberty, and one’s right to one’s body. Some examples containing the theoretical traits are:
Luka v Lowrie, 136 N. W. 1106, Michigan 1912: A child, who experienced a crash injury to his foot, was deemed by the surgeons that amputation was necessary. Normally, a child would not be considered to have competence for consent, therefore the parents should grant consent to the surgery. However, the parents were unavailable for discussion during the duration of the surgery. Without consent, the surgeon, after consulting with several physicians, performed the amputation. From this case, it can be justified based on act utilitarianism, where the goal of an action should be to achieve the maximum amount of happiness. Had the surgeon acted in a strong deontological view, and that the surgeon absolutely respects individual liberty and consent, the child’s situation may have turned another way.
In re Melideo, 390 N. Y. S. 2d 523, New York, 1976: Mrs. Melideo received a dilatation and curettage of the uterus for diagnostic purposes. The patient developed significant bleeding soon after. The patient however, refused blood transfusions based on her religious belief. The court ultimately ruled that blood transfusion should and was not ordered to the patient, since the patient has consent competency. This follows the patient centred deontological view, where certain rules are unethical to be broken no matter the circumstances, and the patient has the ultimate right. Interestingly, in this case, there are two layers of deontological reasoning present. The first layer exists in the surgeons who acts as the “agents”. The surgeons respected the rule for a patients’ liberty based on the patient centred deontology, and the patient followed the basic deontology view where the decisions should never break certain rules laid upon oneself.
The two cases above represented how the two views can be at play at the same time instead of counter arguing. The deontological approach respects one’s autonomy and liberty, while the utilitarianism view fulfils certain situations where emergency consents are needed. Murray confirmed this in one of the conditions for emergency consent: the proposed treatment is for the ultimate benefit of the patient.
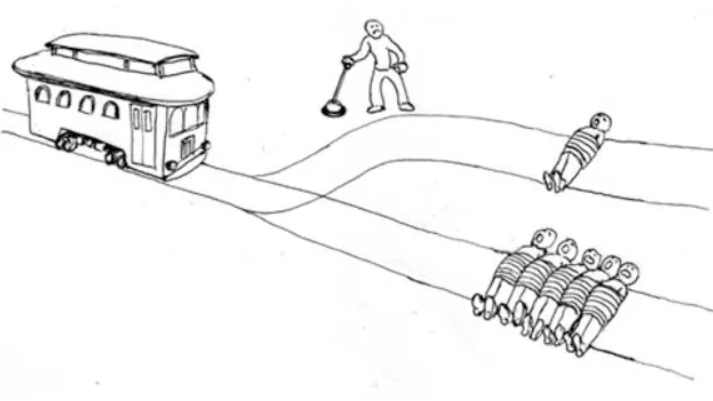
One possible reasoning for this might be the importance of liberty from both viewpoints. In an action-based context, such as the world-famous trolly cart problem, where 5 people will die if you don’t push the lever, and 1 person will if you do, the deontologist will not push the lever, only if the person has a doctrine to never kill in their mind. The utilitarian will push the lever for the maximum amount of happiness. This may make the utilitarianism seem like a violation of some individual liberties in some cases.
However, in the context for information, Mill argues that even though some truth may result in harms, they should still not be suppressed. The reason for this is that Mill follows the empiricism of knowledge, that knowledge can only be gained by experience, and that future knowledge (or truth) cannot be known. Therefore, suppressing the truth will assume its infallibility, which contradicts to Mill’s empiricism. This also supports the importance of information transparency to the patients so construct patients’ well-rounded judgement toward the procedure.
“Had the patient, judged as a reasonable and prudent person, been provided adequate information about the procedure and its risks prior to consenting to the procedure, or if some material risk had been presented, would the patient have refused to proceed with surgery?”
This leads to another philosophical debate on free will and determinism. From the determinism point of view, Paul Ree is an example, that he holds a hard deterministic view. Ree believes that every decision was made from past events, and that an association of causation is present. Ree also argues that free will is an illusion since the causes are internal. For example, when a rock was thrown, the causation was observable, and it is external. Those events can be replicated and proven, given the exact force applied and other factors such as wind speed. To say that the rock has free will would not be plausible. From this logic, internal factors such as body chemistries or past experiences leads to determined behaviours of a person or an organism. Ree gave the example of a donkey between two of the same haystacks. If the donkey was observed to turn left and eats the left haystack, externally, it would seem like the donkey has free will, but what about hidden factors? The wind may be blowing towards the donkey from the left side, or a hidden body behaviour gathered from past experiences. Therefore, since some factors were internal and unobservable, and created the illusion. Ree believes that if the exact past causation, both internal and external were recreated to the exact same extent, the donkey would still choose to turn left. Same as when a person makes certain decisions.
While not many philosophers support purely on free will, many of them believes that free will and determinism can exist at the same time (Compatibilism). Compatibilists argue that if only causal determinism exists, there won’t be any needs for moral responsibilities. Since determinism argue that only one path was available to the person, and that person must act in that way. Therefore, there isn’t a responsibility for that person’s action. To apply moral responsibilities then, free will will be required. For compatibilism, theories vary. But Fischer’s (1994) theory can provide a supporting ground for information transparency in medical consent. Fischer provides an element called regulative control which is a control agent that can bring and refrain one from doing certain behaviours. As a result, different paths open for one to choose at that exact moment. For medical consent, the importance for surgeons to provide patients a clear view of the procedure surfaces. Therefore, the compatibilist view justifies the need for risk disclosure that it provides the patients a clear, rational judgement when they are competent for consent.
From the example and arguments above, medical consent is constructed on the foundation of individual liberty. While it can be fitted into many different philosophical debates. For novel medical research, personally I would argue for the respect of liberty and autonomy, and transparent communications for patients to create rational and justified decision. Yet, certain context may prove otherwise and incite debates.
From beginning this module, I was exposed to various different topics all under the field of engineering replacement body parts ranging from ethics in research to orthopaedics. However I was surprised to find myself knowing nothing about tissue engineering until the lecture we had on it had taken place. Which was what had inspired me to do some research on the topic.
WHAT IS TISSUE ENGINEERING
Falling under the field of regenerative medicine, tissue engineering bares the goal: to assemble functional constructs that restore, maintain, or improve damaged tissues or whole organs.
It could potentially be used in surgeries in which necrosis (premature cell death in tissues) occurs. It has very considerable potential, for which scaffolds from human tissue are thrown away because of necrosis, and in combination with a patients own cells, could make synthesized organs that won’t be rejected by the immune system.
Because tissues are groups of cells grouped together, its obvious there would be certain cells needed so that tissue engineering can be brought about, the types are:
Adult/fetal cells
Adult/fetal stem cells
Pluripotent stem cells
And these cell sources can be divided based on their origin:
Allogenic cells- from a human donor
Autogenic cells- the donor and recipient are the same
Syngenic cells- from an identical twin
Xenogenic cells- from an animal
Allogenic cells – Adult cells- currently have greatest clinical use – Using fibroblasts which come from banks (of human donors) – Available commercially Have a high growth potential
Autogenic cells – Involved biopsy of cartilage (examination of sample cells from a patient to determine presence/extent of disease) – From which chondrocytes are isolated and cultured, then implanted (with a biomaterial) back into a damaged joint to form a functional cartilage – But its controversial and has mixed results
Syngenic cells Aren’t used commercially
Xenogenic cells – Aren’t used commercially at all – Hybrid embryos are allowed to be created
Table summarizing the 4 origins of cell sources
TISSUE ENGINEERING IN PRACTICE
A science paper published on the National Institute of health mentions: “currently, tissue engineering plays a relatively small role in patient treatment. Supplement bladders, small arteries, skin grafts, cartilage, and even a small trachea have been implanted into patients, but the procedures are still experimental and very costly. “
This means, they have been successful in implanting small tissues into patients, however it comes at a price. On the other hand, more larger organ replacements like the heart and lungs, although have been successfully synthesized in the lab, have yet to be successful in replacing the organ in a patient. But steady progress has been made.
From another point of view:
A different means in which tissue engineering can provide a useful solution in is plastic surgery:
another paper published by the National Institute of Health mentions:
“As a group, reconstructive surgeons are facing more challenging composite defects than ever before coupled with internet and media savvy patients with increasing expectation.”
And goes on to say:
“Among these approaches, the most attractive concept is tissue engineering.”
Indicating in order to overcome the increasing expectations of patient’s expectations, and the number of potential patients in the future, by using the concept of tissue engineering. They can meet these demands, and “restore both form and function” to the area in which surgery takes place.
CONCLUSION
To conclude, tissue engineering has brought about potential solutions to various issues in both the medical and cosmetic field. Ranging from lack of potential donors in both of these fields (which means they won’t have to standby and wait for donors in transplant surgeries), to overcoming the severely high demand to of potential patients in the future expecting full restorations in reconstructive surgeries. Meaning, tissue engineering could become a key in which modern medicine can be revolutionized.











This is an initially reflective and well researched blog showing how you have chosen to explore the emerging field of…
This is a good attempt at a blog, where you reflect on your recent learning at a lecture/workshop to describe…
This is a fair to good blog, reflecting on your recent learning in some of your modules. You provide a…
This is an engagingly written and reflective blog focussed in general on ethics in medicine. You might improve by citing…
This is a good and well written an presented blog on an original subject - biofilms on implants. You explain…