After a long day of lectures, my housemates and I decided to watch a couple of episodes of Black Mirror on Netflix. This is an series based on the dangers of technological advancements in a dystopian near future. The scary aspect of Black Mirror is that the rationale and vision for these technological advancements portrayed in the series is highly compatible with our own. Even with good intentions such as curing disease and reducing crime, brings its own consequences.
We watched an episode whereby all your memories were recorded so that you could watch them back or could be used by police and authorities. In the show, it was originally designed to help with those suffering with Alzheimers, but now has evolved into something more sinister than intended. It brought up an ethical debate within our house on whether or not we would do it, as well as the topic of free will.

We discussed that very few have an issue with prostheses to help with motor functions such as hip and knee replacements, prosthetic legs, and even replacement organs such as a pacemaker. However, what about prostheses in the brain? I am a Neuroscience student and realised there were very few examples of neuroprosthesis so, naturally, I was intrigued. The brain is one of the only organs in the body where we cannot get a transplant, and this is only explored in science fiction.

What are the current technological possibilities?

Elon Musk is currently developing a technology called ‘Neuralink’ that will give people with quadriplegia the ability to control computers and mobile devices with their thoughts. Fascinating!
https://neuralink.com/ – Read more about their approach and applications
Here is a podcast discussing the current breakthroughs in commercialising Brain-Computer Interfaces using a minimally implantation method and a soft electrode device. They explain how they received lots of support in the early stages of research, showing it to be an area of interest for investors. Their approach is to build on existing research and translating that into clinical practice.
Next Steps…
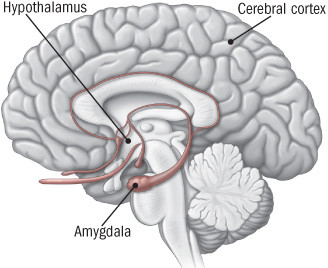
If our liver stopped working, we could use stem cells, and get a transplant, and there is even research regarding a 3D-printed liver. What about the brain? For an Alzheimers or Multiple Sclerosis patient, would you consider using stem cells or an implant to replace parts of the hippocampus or myelin for neurons? Yes, most likely. What about someone with Schizophrenia, would you replace their frontal or temporal lobes? What about depression, autism, ADHD or OCD? By definition, they have an illness or a disorder.
Where would we draw the line?
Discussion point:
Imagine someone in the army or someone who has experienced trauma. Prosthesis is a way of improving someone’s quality of life, so how far can we go? Would we attempt to make people less emotional, smarter, remove traumatic memories, and stop people from experiencing fear? This would certainly improve their capabilities as a soldier, improving their quality of life and removing the risk of developing PTSD, experienced by many soldiers.
Is this improving their quality of life or eradicating a vital part of their identity?
How would society change if this was the norm?
Here are 2 episodes of Black Mirror that show the applications of neural implants that go beyond treating neurodegenerative disease…
My final thoughts:
I believe that neuroprosthesis should be encouraged as it could change millions of lives for the better. Only with strict regulations can these advancements benefit society and help those suffering with physical and mental health problems. I don’t belive that society will be benefitted from technology enhancing memory, intelligence or physical capabilities in those who don’t require serious help or assistance.











This is an initially reflective and well researched blog showing how you have chosen to explore the emerging field of…
This is a good attempt at a blog, where you reflect on your recent learning at a lecture/workshop to describe…
This is a fair to good blog, reflecting on your recent learning in some of your modules. You provide a…
This is an engagingly written and reflective blog focussed in general on ethics in medicine. You might improve by citing…
This is a good and well written an presented blog on an original subject - biofilms on implants. You explain…