Following our lecture on tissue engineering, I researched new techniques in tissue engineering and read an article on a woman who had a 3D-printed ear implanted using her cells after being born with a misshaped ear. It’s the first clinical application of 3D bioprinting.
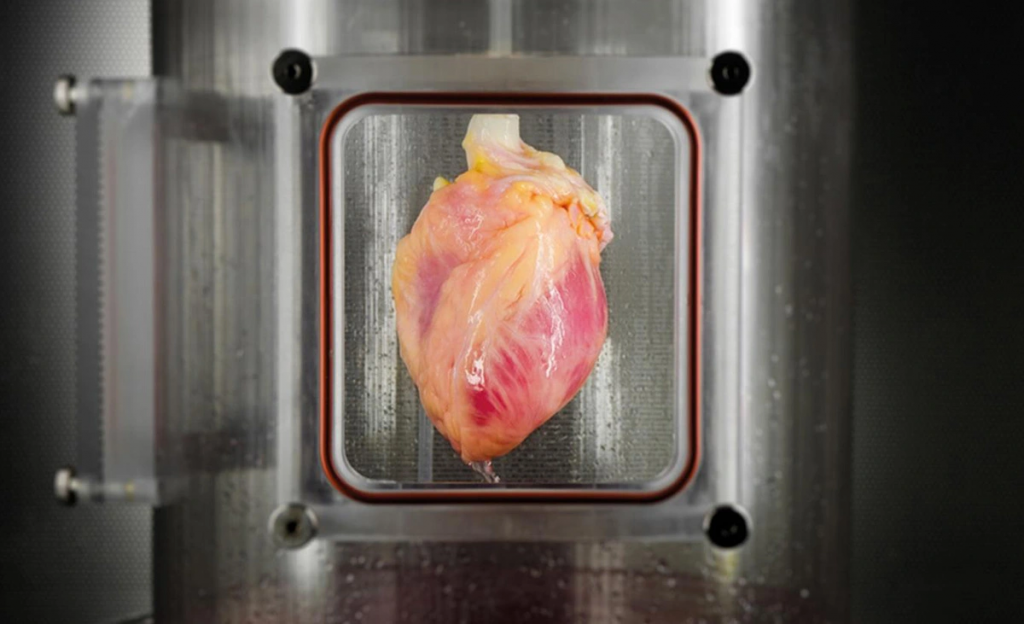
The current goal of researchers is to develop more complex organs like hearts ready for transplant in the next 10 – 20 years. With a shortage of organs to transplant patients and nearly 7000 on a waiting list in the UK alone, the impact 3D bioprinting could have on organ transplantation is immense. It’s crucial progress towards personalized medicine that improves patient outcomes by reducing the risks associated with organ transplants.
As someone interested in working in the pharma industry, I was curious about the issues regarding the ethics of 3D bioprinted organs since all emerging biotechnologies must be ethically assessed before clinical use. Organ transplant currently creates a vast range of ethical dilemmas, so what would happen if we add artificial organs to the mix?
How it works
Although I won’t go into detail on the technique of bioprinting, it’s interesting to learn how 3D printers can print human tissue. Bioprinting relies on bio-ink, comprised of living cells surrounded by hydrogel molecules and acts as a digital file. Once loaded into the cartridge it’s deposited layer by layer of living cells to form 3D human tissue. It’s then crosslinked to become more stable by UV light or ionic solution, allowing it to grow and develop into a functional human organ.
Ethical Issues
The development of 3D bioprinting from laboratory to clinic brings with it established ethical concerns, such as the source of cells. Stems cells are widely used cell source obtained from living or aborted fetuses, raising a bioethical debate to determine their moral status, making their use heavily criticized. Xenogeneic cells are another option as a cell source, although their use has societal and religious concerns, and research has also shown there are psychological issues related to identity for xenotransplant patients. Personally, as a Muslim, I would object to an organ printed using pig cells and would be more inclined to an organ made from my cells. It eliminates the burden of knowing that another person died to save your life, as not all organs can be collected from living donors.
The clinical translation of this technology also brings emerging ethical issues related to personalized medicine to the forefront. Introducing 3D bioprinting into practice requires clinical trials. Generally, trials for 3D bioprinting involve testing patient safety and efficacy of the treatment using randomized placebo-controlled clinical trials e.g. (CAR T cells). Theoretically, it’s possible to test uncertainties related to the risk of harm to a limit, using small transplantable tissue. However, 3D-printed organs made from autologous cells are designed specifically for a patient, making it impossible to extrapolate the results from a randomized clinical trial. Ultimately the patient would have to be their own lab rat.
In addition, due to the invasive nature of the treatment the patient’s right to withdraw as a study participant is challenged. Since the reversibility of organ transplantation is limited, without causing harm to the patient and significantly impacting the chance of alternative treatment. It’s a critical issue for a patient to lose access to better treatment in the future because they participated in an experimental trial. Also, as an experimental therapy, it’s difficult for a healthcare provider to disclose all of the risks associated with treatment. So, even if the patient is conscious and has the capacity they might still not be able to provide informed consent.












This is an initially reflective and well researched blog showing how you have chosen to explore the emerging field of…
This is a good attempt at a blog, where you reflect on your recent learning at a lecture/workshop to describe…
This is a fair to good blog, reflecting on your recent learning in some of your modules. You provide a…
This is an engagingly written and reflective blog focussed in general on ethics in medicine. You might improve by citing…
This is a good and well written an presented blog on an original subject - biofilms on implants. You explain…