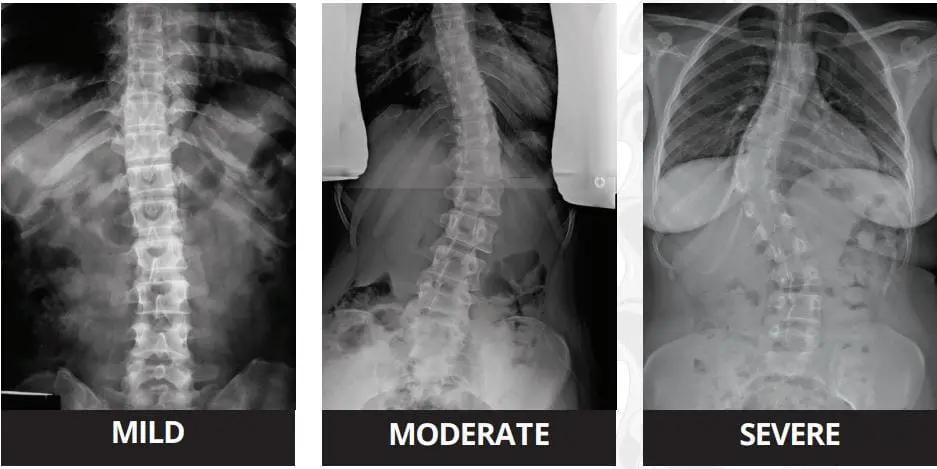
Scoliosis is an abnormal lateral curvature of the spine, causing misalignment. In order to be considered true scoliosis, the curvature, measured by the Cobb angle, must be more than 10 degrees. Spine specialists recommend different treatment options depending on this angle, with more severe and progressive cases resulting in surgery.
Spinal Fusion
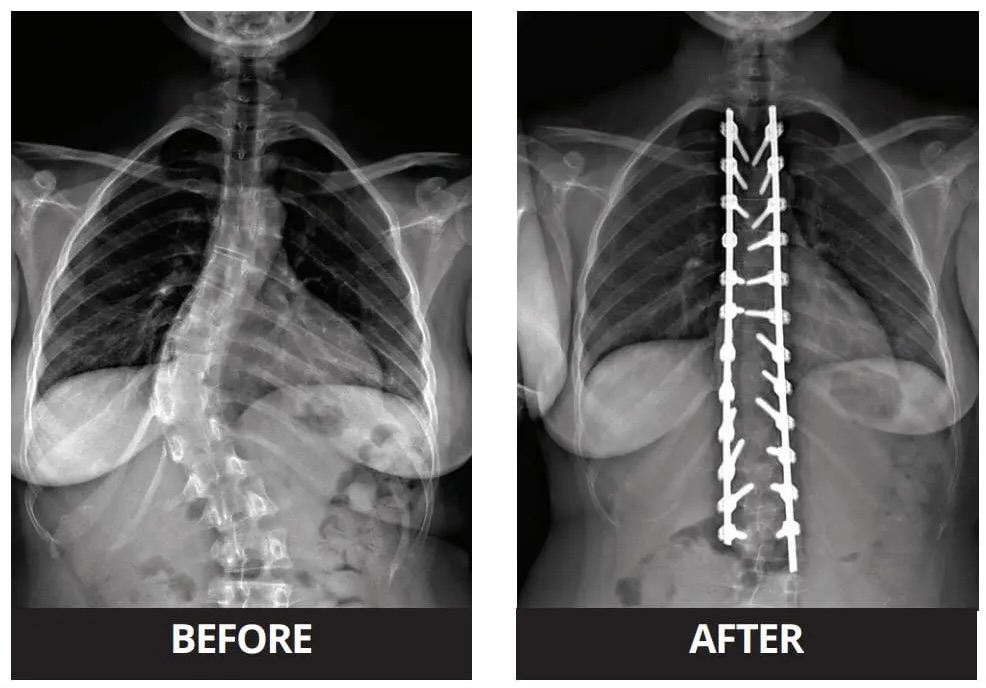
Spinal fusion, which has been the standard surgery for scoliosis for the past century, involves realigning and fusing the curved vertebrae with screws and rods. Although this procedure has good outcomes, with low complication and re-operation rates, it can diminish spinal mobility and flexibility. This means that those taking an interest in sports who undergo spinal fusion, for example, can lose their ability to perform. As someone with scoliosis myself (although mild), and having previously competed in tennis tournaments, this got me thinking about alternative spinal surgeries that do not have a negative impact on mobility.
“The desire to maintain spine motion has fuelled the development of various growth modulation procedures. The goals of these procedures are to correct the spinal deformity and maintain motion.”
Scott. J. Luhmann, M.D.
Vertebral Body Tethering
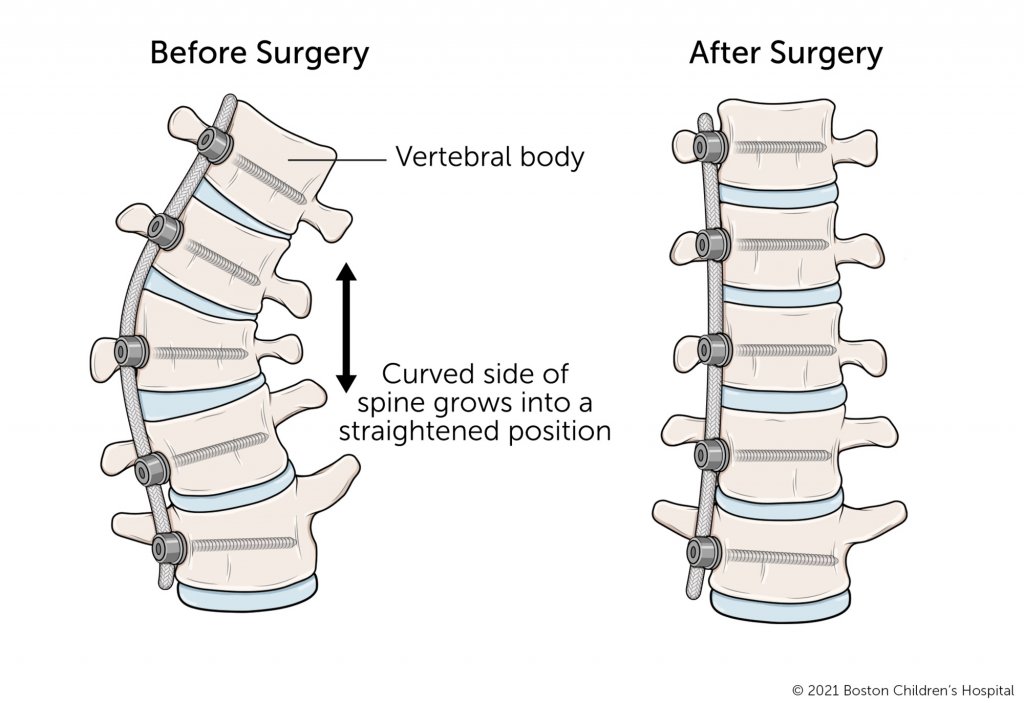
As of recent, non-fusion spinal surgery has been used on those with scoliosis to correct curvature, while preserving flexibility and mobility. One method is through vertebral body tethering (VBT). This is where anchors (coated in hydroxyapatite, the substance that bones are composed of) are anteriorly attached to the vertebrae on the convex side of the scoliotic curve, with a flexible tether (made from polyethylene-terephthalate) connecting these anchors. The foundation of the procedure is that the tension from the tether slows the growth on the convex side of the spine, giving time for the concave side to catch up and driving the spine into the correct alignment. Due to the flexibility of the tether, and the absence of bone fusion, this allows for better spinal mobility post-surgery. Because VBT works via growth modulation, the most suitable candidates are those who have yet to reach skeletal maturity or are experiencing progressive scoliosis. This therefore means that VBT is less generalised than spinal fusion, and due to it being a new approach, there is some uncertainty with its long-term outcomes. Possible complications surround the fact that the tether may break through prolonged stress, though this does not pose much of an issue once spinal correction has completed. Early reports into the post-operative results of VBT do however demonstrate a high success rate and low revision rate.
Posterior Dynamic Correction and The ApiFix
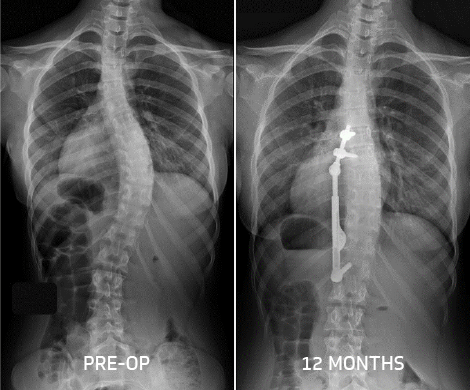
Another non-fusion surgery for scoliosis is posterior dynamic correction, which occurs with the use of the ApiFix. The ApiFix is a self-adjusting rod, implanted on the concave side of the spine using a posterior approach, serving as an internal brace, and helping straighten the spine. The device can expand and so accommodates skeletal growth and additional correction. It is fastened to the spine with a single-level fusion (meaning only two vertebrae are being fused), with a total of only three screws needed. The rod features two polyaxial joints in which the vertebrae are fused, providing a greater degree of motion than spinal fusion. The ApiFix is most suitable for those with single spine curves and a Cobb angle between 35 and 60 degrees. Because this device and the procedure is novel, questions have arisen about its success rates. For example, possible complications include rod breakage and osteolysis (destruction of bone tissue). Early reports into the post-operative results of posterior dynamic correction with the ApiFix do however display its success and provides preventative measures to decrease failure and re-operation rates.
Final Thoughts
As I researched into the topic of surgical treatments for scoliosis, I was pleased to find other options as well as spinal fusion that can help preserve the individuals spinal mobility and flexibility. I believe that it is important to offer various treatments, while considering patient suitability, in order to improve the patient’s condition while not having a negative impact on their lifestyle. With the nature of these procedures, it has given me insight into how individuals requiring scoliosis corrective surgery have to negotiate between greater spinal motion with some uncertainty in long-term outcomes, or a long-lasting solution with diminished spinal motion. Personally, I would decide to go with the former option, with spinal fusion becoming a last resort if long-term outcomes are not successful. Nevertheless, I am excited to observe the follow-up results of these newer procedures and the advances technology will have on scoliosis corrective surgery.