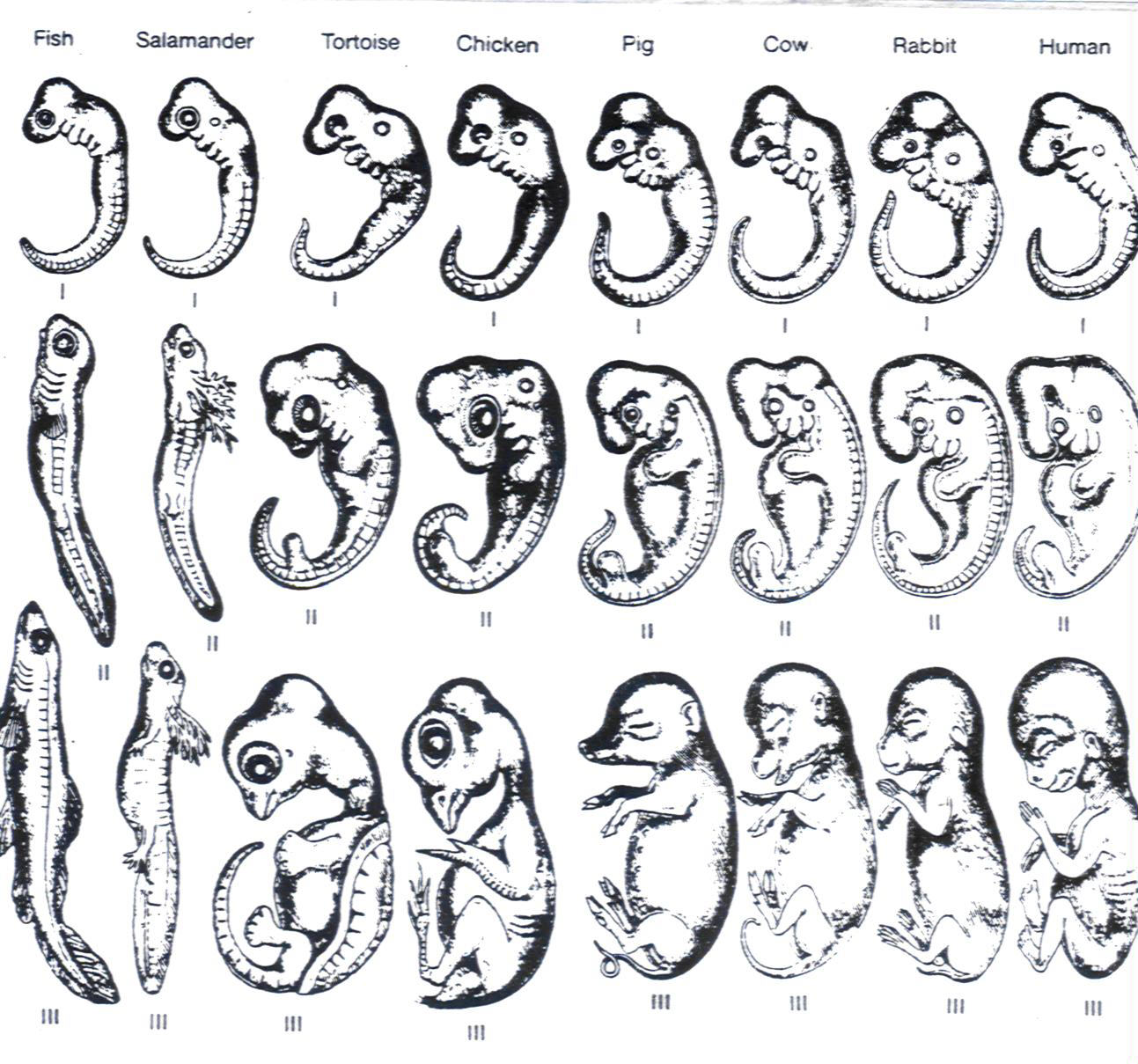
During a debate session on embryo testing and the fourteen-day rule, an argument was raised in favour of scrapping all testing on human embryos; the claim was that, in the early stages of embryo development, vertebrates have “deep structural similarities“, so animal embryos can be used in place of human ones for all relevant research.
The claim that animal and human embryos are indistinguishable enough that animals can be considered ‘good enough’ for human research is a debatable one, but this was not what stuck with me after the debate session. I found myself unsettled by the ease with which “let’s just use animals” became a conclusion from those who supposedly value life enough to argue against embryo testing in its entirety. It seemed contradictory to me; a pro-life stance displayed unexpected double standards concerning the morals surrounding humans and other vertebrates.
Though my current degree is in biomedical engineering, my future goal is to pursue a career in veterinary medicine. I have had pets from a young age and believe the companionship and trust of an animal to be one of the greatest experiences available to us in our lifetime. Part of my decision to take this module is my long-term interest in the work of Noel Fitzpatrick on developing prosthetic limbs for animals, hence saving the lives of pets who would otherwise be put down, or not afforded the same care that a human patient would be. I value life regardless of species, and as a consequence, lean towards standing against animal testing.
Animal testing for medical research is an extensive field, ranging from the aforementioned embryo research to tests on conscious animals, where many are subject to deliberate harm. I am struggling to type this section of the post and am procrastinating on my research into the details of animal testing. I cannot bring myself to insert images I’ve seen from secret surveillance of testing at Wickham Laboratories. My impulse reaction is to condemn it for its cruelty. For the most part, a human has a choice. An animal does not.
Naturally, the ethical debate is heated. Many organisations oppose all animal testing and strive to eradicate it; their websites are full of stock images of animals in cages that make me want to shut my laptop and perhaps switch to a humanities degree. It is also a highly profitable industry, which, in the realm of medicine, is a statement that should always sound alarm bells. Some claim animals should be afforded the same rights as humans, as “individuals with inherent value“.
Whilst I am no vegan, I am inclined to agree in the context of the suffering undergone in many animal testing regimes. Even my word choice here should be considered; the distinction between ‘human’ and ‘animal’ is being made when it could be argued that we are one in the same. I am using these words for ease of communication, but whilst I write, am considering whether I truly believe this separation to be just.
Of course, the benefits are numerous and significant. Eradication of certain diseases, such as smallpox and polio, has been achieved through animal testing. As a notable example, eradication of AIDS is on the horizon. Animal research has developed our understanding of transplantation, anatomy, biological systems, behaviour, pain, and memory, to name but a few. Some benefits cannot be replicated in human alternatives, such as the availability of a shorter lifespan, where the effects of procedures or drugs on an organism can be observed over a whole life cycle and experimental times can be shortened.
The role of non-human animals to serve our betterment as a species is a viewpoint that can be found as far back as the Bible. Christian theologians support a hierarchy of animals, and it is not difficult to see how this idea, in the cultural Christianity of the Western world, remains an influence on the ethics of animal research.
(Once again, I view this as a stance contradictory to another argument that Christianty backs up using faith: that abortion is immoral, since life begins at conception. How does one religion support the rights of a handful of cells to such an extreme, whilst condemning non-human animals as simply tools of humanity? But that is an issue to tackle another day.)
I have spent many a weekend in the library over the course of my degree. This one is by far the most intense. I cannot hope to organise my thoughts on the whole topic of animal testing in one sitting, with nothing but my Thermos flask of tea as emotional support. Hence, I will consider a scenario where the issue of animal testing has directly affected me.
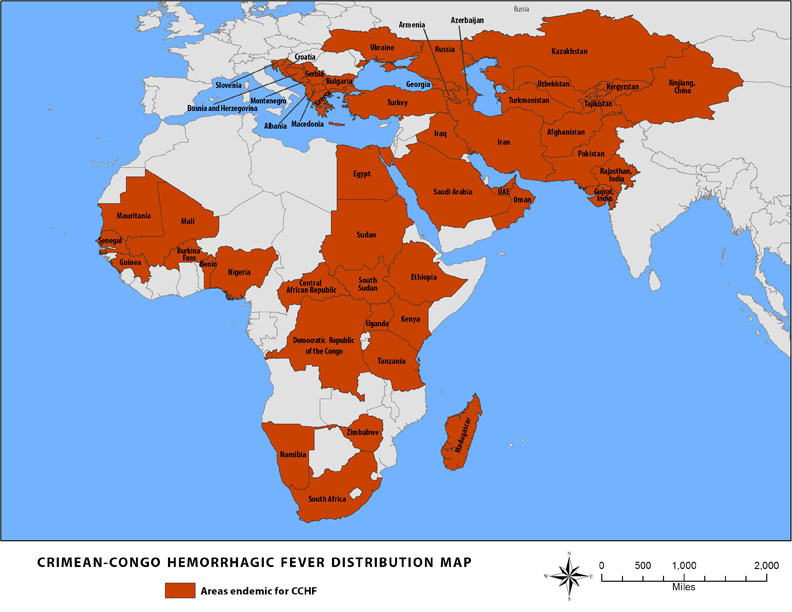
Crimean-Congo Haemorrhagic Fever
Since February 2024, I have been involved in the first phase of human clinical trials for a vaccine against the virus causing Crimean-Congo haemorrhagic fever (CCHF). It is endemic in regions the primary tick vector is native to, but has spread further due to animal-to-human and human-to-human transmission. Outbreak fatality rates vary depending on the source, but the NHS suggests a fatality rate of up to 80%. Readers may aready be aware of the CCHF virus; in 2023, concerns rose about its imminent spread across Europe, and its trajectory towards the UK.
It is clear that this virus is a pressing concern. Phase one of the human trials for the MVA-based vaccination were recently begun by the National Institute for Health and Care Research; I joined the study as a healthy volunteer at the Southampton Clinical Research Facility, receiving two doses of the vaccine with monitoring of my immune response throughout. My final session was completed on Tuesday 18th March 2025.
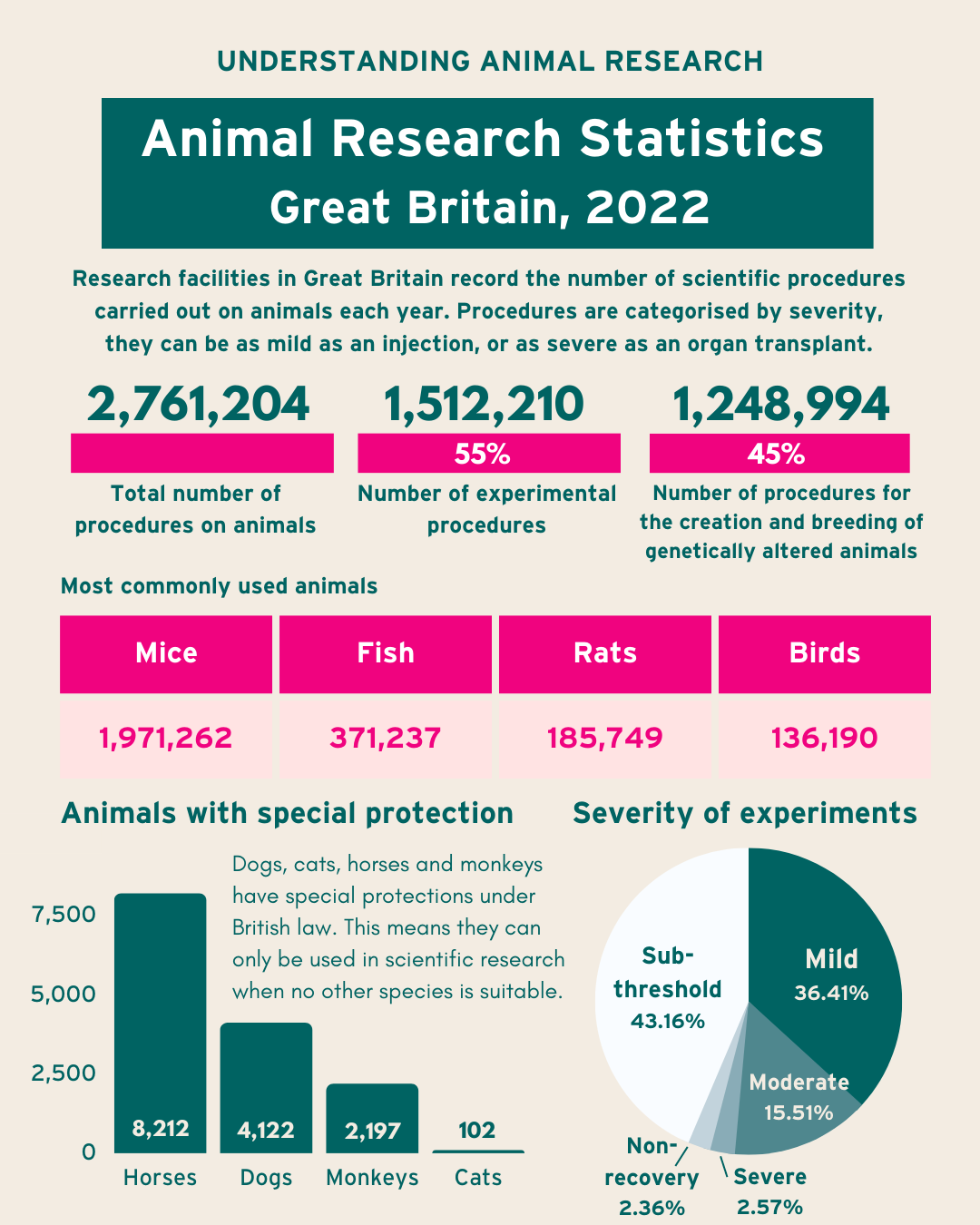
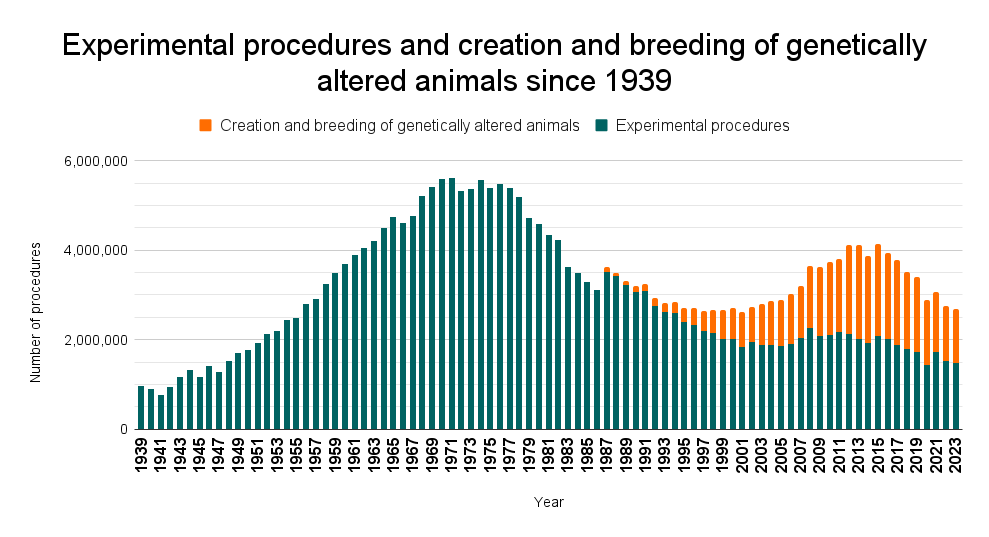
Animal testing often precedes the human phases of a drug trial. According to the RSPCA, who advocate for human alternatives wherever possible, around 5 million animals are used annually across the EU alone for research into medicine and vaccinations. This is a hot topic; in 2023, the US government ruled that the FDA no longer required animal testing for new drugs to be approved. A recent study claims that only 5% of animal tested drugs make it to market, and there is evidence to suggest the ineffectiveness of animal testing in pre-clinical trials. Detached from my own experience, I would consider this information and maintain my anti-animal testing opinions. I would consider if it was truly necessary; when other pre-clinical tests and human alternatives are available in drug development, are we making a justifiable sacrifice? Knowing myself and my weaknesses when confronted with the suffering of vulnerable creatures, I would likely conclude, no.
The use of animal testing for the CCHF virus vaccination was confirmed to me from the first day of my involvement, when I read the participant information form. A casual line in the middle of this lengthy document states: “Data from pre-clinical animal studies show that MVA-CCHF is effective at inducing an immune response.”
I had no symptoms or side effects from the vaccination. According to the nurses on the study, the same was true for all other participants in my group of the first phase. But who—or what—did suffer side effects, or worse? Not once in the year-long trial process did I consider this, until now. The only vague memory I have of a reaction to the animal testing information, when I read that line for the first time, was reassurance.
As I type in level 3 of the Hartley Library, I wonder if I can allow myself to feel guilt.
It is one thing to take a stance against animal testing, and quite another to wait for an experimental vaccine to be administered to you, with little knowledge of the potential side effects—only the fact that other living creatures have already received this and it has been deemed safe enough to give to you, a member of a species whose lives are undeniably valued above all others. I lost count of the number of medical personnel who surrounded me on each injection of the vaccine. The research facility must now have enough of my blood to fill a small swimming pool. When the curtains are drawn around you and you spend the next four hours under the watchful eyes of multiple nurses, your vitals checked with unsettling regularity, it is difficult to think of anything besides your safety. Is this response selfish? Here, too, I would argue no.
Now my involvement in the trial is over, I can look back on my experience and question whether I would have taken part without the knowledge that the vaccine had passed animal trials. I have considered the scenario where they hadn’t been performed, and my phase of human trials was therefore the first test on a living organism. As a student of medical sciences, I should be able to look critically at other information—such as the previous success and safety of MVA-based vaccinations—to make a decision. But no detached, logical assessment would be enough to stamp out the instinctive fear that comes from being injected with an unapproved drug. Without that line in the information sheet, it is likely that I would not have taken the risk.
I have no diagnoses that affected my participation. I consider myself confident with my health. I had no issues with the process of the trial—quite the opposite, since I find blood tests enjoyable. It was academically interesting to me; I got to experience an ECG test in the same month in which I completed an ECG lab project. The reimbursement was an indisputable temptation for a student with concert tickets to pay for. If I, the perfect fit for a clinical trial volunteer, would be put off by the lack of animal testing, then so would many others. How much longer would it take to develop the CCHF vaccine with this drop in volunteers and likely necessity for longer, more tightly controlled human trials? Would we see a spread in the meantime that would lead, as headlines claimed, to the next pandemic? These are extreme hypotheticals, but they are conceived through consideration of my own double standards.
A Tumultuous Attempt at Conclusion
Harvard Medical School belives animal testing to be “a privilege,not a right,” a statement with which I now agree. I have been afforded the privilege of safety and consolation, protected from unrealised side effects and health paranoia behind those animals who, like me, received an experimental drug.
I will keep up to date with progress on the treatment of the CCHF virus. Drug trials are a lengthy process, and by the time the vaccination is approved, I might be a qualified vet. I would take every moment of the care of an animal to be a blessing, but so too would I take the successful treatment of a deadly disease as one. I am left with a new appreciation of the necessity of animal testing after the first-hand realisation of how eradication may not be achieved without it.
Whilst I wrap up this post, I realise I have exceeded the word limit substantially. If I were to remove large chunks of text as required, I would lose important details of the thought process that has spanned many hours since the embryo testing debate to my final trial session last week, and that will stick with me far beyond the submission date. I am politely requesting permission from the examiner of this work to allow me this infringement.
I can conclude that my opinion on animal testing has been rendered more complex, and would like to state another realisation that I hope will be considered for the future of this module: when communicating a reflective process on the subject of medical ethics, five hundred words will never be enough.
Photo: (left to right) my pets Lola, Ginger, and Tommy, the latter of whom I have loved and looked after for seventeen years, and whose appearance on my phone lockscreen made me tear up whilst writing this post.
The use of microbubbles within cancer treatment sounds comical, but these little bundles of joy can be used for a variety of medical applications. Over the last decade, these have been praised as the future of Cancer diagnosis and treatment and represent a safe and non-invasive alternative to Chemotherapy. I first heard about Microbubbles at a Workshop as part of my University, and it fascinated me that Microbubbles could kill cancer cells while sparing healthy ones, unlike Chemotherapy. This piqued my interest, which made me want to learn how they can be used to treat cancer within patients.
What are Microbubbles?
At the Workshop, I learned that Microbubbles are small bubbles (0.5–10 μm) consisting of a phospholipid outer layer and gas core and are used clinically during Ultrasound Imaging. When injected during Ultrasound Imaging, they resonate vigorously under the transducer, reflecting waves more effectively in body tissues and increasing imaging sensitivity.
However, once researchers realised these bubbles could move around the body safely, drug delivery in the treatment of cancer was greatly considered.
So Why Are These Tiny Bubbles So Effective In Treating Cancer?
Currently, chemotherapy drugs are injected into the blood and destroy cancer cells, however, this can also result in the death of healthy cells, leading to shocking side effects such as nausea and hair loss.
Microbubbles, on the other hand, can target smaller doses of chemotherapy drugs to cancer cells alone due to their Phospholipid shell, preventing the damage of healthy cells, reducing side effects, allowing patients to recover quicker.
“By using microbubbles and ultrasound we can control when and where a drug gets released, and crucially also distribute it throughout a tumour”
However, within aggressive types of cancer, low oxygen levels in tumours cause resistance to chemotherapy drugs, so to resolve this, Microbubbles can be filled with oxygen to improve the delivery of the drug and its ability to kill more aggressive cancer cells.
I was glad to read that the use of oxygen within microbubbles has also seen some effectiveness in reducing Cancer within rats, however, this is still within the pre-clinical research stage. Overall, there is some promise, but it was shocking to read that a separate stroke study revealed safety concerns when high dosages caused haemorrhaging in two patients, showing that parameters of ultrasound radiation and the number of microbubbles when applied should be evaluated to prevent this from ever happening again.
So Microbubbles May Have The Potential To Cure Cancer?
Despite this, many reports have reported positive results within the use of Microbubbles, giving it the potential to save many lives. At first, I found it comical that Microbubbles could be used to treat cancer, but my mind has seriously changed after reading different articles and papers within this field.
I found it fascinating when Oxford scientist Dr Stride told New Scientist that “If you expose the blood-brain barrier to bubbles and ultrasound, you can temporarily and reversibly enhance its permeability, which is potentially interesting for a lot of brain treatments”, which made me believe that Microbubbles deserves further research as it may also have the potential to protect brain cells from dying. I’m excited to witness what I’ve called the ‘bubble revolution’ taking shape within the NHS, and seeing the countless lives that will be transformed thanks to this ground-breaking research.
“Combining oxygen-carrying microbubbles with ultrasound-triggered delivery to solid tumours is a novel approach to enhancing tumour oxygenation and sensitivity to radiation, and it deserves further study,”
Dr. Bernhard Eric Bernhard, Ph.D., chief of the Radiotherapy Development Branch in NCI’s Division of Cancer Treatment and Diagnosis.
says CP. What are Microbubbles? [Internet]. News-Medical.net. 2018. Available from: https://www.news-medical.net/life-sciences/What-are-Microbubbles.aspx
New Portfolio. Editor’s choice: microbubbles [Internet]. Nature. 2022 [cited 2025 Mar 27]. Available from: https://www.nature.com/collections/edfggagdej
NCI Staff. Using Oxygen “Microbubbles” To Improve Radiation Therapy – National Cancer Institute [Internet]. www.cancer.gov. 2018. Available from: https://www.cancer.gov/news-events/cancer-currents-blog/2018/microbubbles-radiation-breast-cancer
Medeiros J. Using microbubbles to target cancer tumors [Internet]. WIRED. 2017 [cited 2025 Mar 27]. Available from: https://www.wired.com/story/cancer-bubble/
Hu Q, Zhang Y, Fu L, Xi Y, Ye L, Yang X, et al. Progress and preclinical application status of ultrasound microbubbles. Journal of Drug Delivery Science and Technology [Internet]. 2024 Feb [cited 2024 Oct 2];92:105312. Available from: https://www.sciencedirect.com/science/article/pii/S1773224723011644
Spencer B. The tiny bubbles filled with drugs that could transform cancer treatment [Internet]. Mail Online. Daily Mail; 2015 [cited 2025 Mar 27]. Available from: https://www.dailymail.co.uk/sciencetech/article-3123944/The-tiny-bubbles-filled-drugs-transform-cancer-treatment-Findings-reduce-effects-chemotherapy.html
Macrae F. Bubbles “could deliver stroke drugs directly to the brain” [Internet]. Mail Online. Daily Mail; 2010 [cited 2025 Mar 27]. Available from: https://www.dailymail.co.uk/health/article-1328644/Bubbles-deliver-stroke-drugs-directly-brain.html
Rumney R. Workshop – Stem cell regenerative medicine – Robin Rumney [Internet]. Blackboard. 2025 [cited 2025 Mar 27]. Available from: https://blackboard.soton.ac.uk/ultra/courses/_228111_1/outline/edit/document/_7135192_1?courseId=_228111_1&view=content&state=view
“Memory is not just the imprint of the past upon us; it is the keeper of what we are, the sum of what we have been.” – Lois Lowry
The purpose of life has been debated for centuries, with many suggesting it lies in making memories- unique experiences that define our identities. But what if those memories fade? For millions of people with Alzheimer’s, memory loss can feel like losing parts of themselves. Inspired by the tissue engineering lecture, I wondered if regenerative technologies could not only restore bodily functions, but also cognitive abilities, such as memory.
Neural implants are showing promise in restoring memories and repairing damaged neural pathways. However, as these technologies advance, they raise significant ethical dilemmas. Could memory restoration extend to memory manipulation? What risks might arise from altering an individual’s memories and, in turn, their identity? This blog will explore the science behind neural implants and the ethical concerns surrounding memory manipulation.
Understanding Neural Implants
Neural implants create a direct link between the brain and external devices, using electrodes implanted in regions like the hippocampus, vital for memory formation and storage [2]. In neurodegenerative diseases like Alzheimer’s, where neural circuits are damaged [3], these implants stimulate affected areas, enhancing synaptic activity and promoting neural plasticity.
What intrigues me is how these devices can learn electrical patterns between neurons, potentially restoring lost cognitive functions. Recent advancements like deep brain stimulation (DBS) and multi-input multi-output (MIMO) systems have shown promise in improving memory and slowing cognitive decline in experimental models. The potential of neural implants to repair and enhance memory continues to fuel my interest in this exciting field.
DBS in Action
An inspiring example of DBS in action comes from the case of an 85-year-old woman, shared in a Medical News Today article which you can find here. After Alzheimer’s caused memory loss, she struggled with daily tasks such as preparing meals. However, after two years of DBS treatment, involving electrodes implanted in her brain to stimulate memory-related areas, she regained her independence. The video below offers a personal glimpse into her journey, offering a testament to the potential of neurostimulation therapies in restoring cognitive function.
As promising as neural implants are for memory restoration, they also raise ethical questions about their potential consequences, especially when it comes to manipulating memories and altering one’s identity.
Manipulating Memory and Identity
Whilst researching neural implants, I encountered an article that touched on the uncertainty of MIMO systems in real life. One concern is how we replicate the personalised selectivity of memory – how do we filter out life experiences that aren’t important, and who decides which memories matter? (Full article here) These questions highlight the ethical dilemmas of memory manipulation, especially regarding identity. In Eternal Sunshine of the Spotless Mind, characters erase painful memories, but the film illustrates the risks of tampering with memory, which could unintentionally erase essential aspects of who we are. With neural implants, the possibility of altering memories raises significant concerns about the control we have over our identities, especially when we are unsure how technology will make these decisions.
Personally, while the potential to help those with memory loss is immense, I believe we must approach this technology with caution. Memory is too central to our humanity to risk losing its authenticity in the pursuit of progress.
Koroshetz WJ, Mucke L. Neurodegenerative Diseases: Where Are We Not Looking for Answers? In: Nikolich K, Hyman SE, editors. Translational Neuroscience: Toward New Therapies [Internet]. Cambridge (MA): MIT Press; 2015 [cited 2025 Mar 27]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK569699/
Neurodegenerative disease has interested me for a while. Having had family with dementia and multiple sclerosis, I’ve known about them from a young age. After Nick Evan’s tissue engineering lecture, I thought about using tissue engineering to treat neurodegenerative diseases. Could we use biomaterials, 3D printing, or stem cells to regenerate lost or damaged neurones?
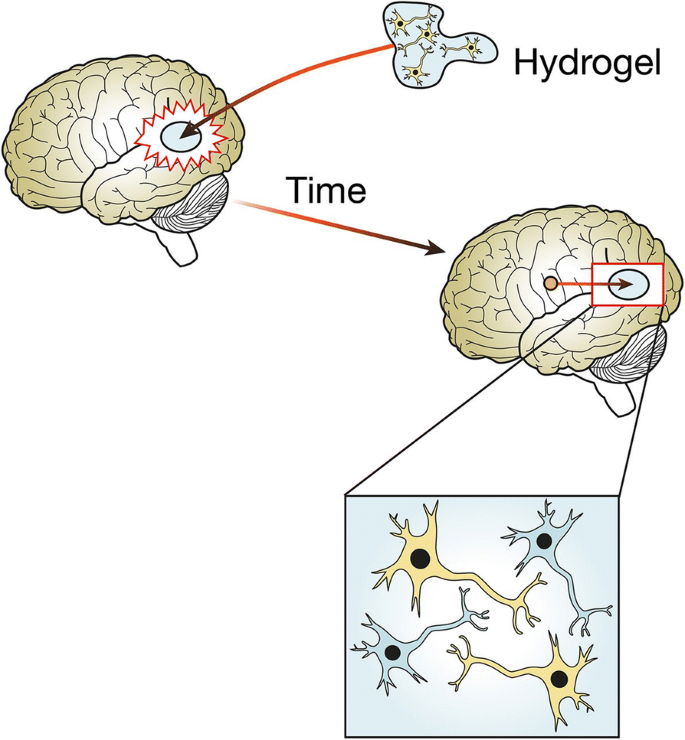
I began to look into how tissue engineering could be useful in treatment of these diseases, and found many approaches. For example, 3D printing bio-scaffolds- structures that allow cell growth and mimic the extracellular matrix. Essentially, a 3D structure which allows neurones to grow in the brain. The scaffold needs to be able to maintain integrity during implantation, not be toxic, allow neuronal migration and proliferation, allow electrochemical communication, and release substances in a controlled manner. One class of materials that looks promising is smart hydrogels. Due to their high water content, they mimic the soft tissue environment and respond to external stimuli. The scaffolds can release growth factors and provide stem cells for nerve regeneration. However, research is still in early stages, as so far, only collagen has been useful for nerve regeneration and hasn’t been implanted in patients. If research advanced, patients with neurodegenerative diseases could have this scaffold implanted to regenerate lost neurones (1).
One unique issue is that the adult brain is designed against neuronal regeneration. Neurones don’t regenerate once they’re lost and there are cell-secreted molecules which make sure of this. Any attempts to regrow neuronal tissue will face this problem and will need to avoid attack from microglia, the brain’s immune cells (2). If you want to introduce foreign material to a brain, you need a strategic and delicate approach.
Another interesting idea I found is that we could create mini-brains from stem cells and engineer them into neurones. This organoid could be used to model diseases like Alzheimer’s and test different treatments on it (3). Alzheimer’s disease is characterised by the build-up of amyloid plaques and tau in the brain (4). With mini-brains, mechanisms can be studied, and drugs can be tested to see if they reduce amyloid and tau build-up. Mini-brains could not only help us understand the disease, but could also be revolutionary for personalised medicine. If we use stem cells from individual patients, a personalised mini-brain could be created, allowing better treatment. This is such an exciting and innovative approach which highlights the possibilities of neural tissue engineering, and if successful in Alzheimer’s treatment, it can be used for other diseases.
What about the ethics?
It is also important to consider ethics in this research. If we get closer to engineering a lab-grown brain, could it have consciousness and feel pain and emotion? Also, current research aims to treat disease and injury, but could it be used to enhance cognitive abilities? Research is still far from these realities, but considering and putting measures in place ahead of time might not be in vain. My research into this topic exposed me to interesting ideas and I will follow the research to keep updated on how neural tissue engineering advances, and how ethics plays into the research being done.
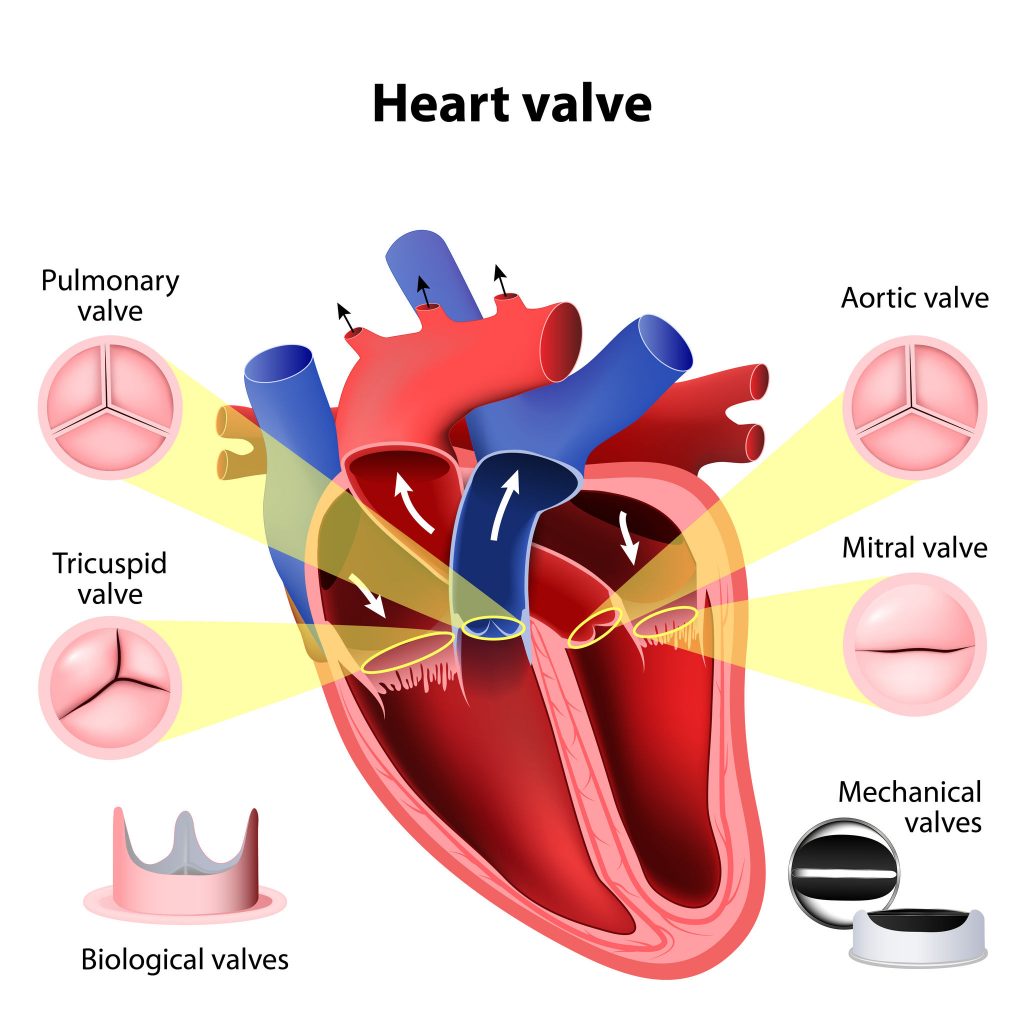
Growing up I spent a lot of time with my nan – something I always noticed was a faint ‘tick, tick, tick…’ coming from her. As I became older, she explained to me this was because she’d had some big surgeries and part of her heart was now made of metal (we used to joke that she was like iron man or the terminator). Her heart valves had become leaky, meaning they had to be replaced with mechanical valves in an open-heart surgery at Southampton General hospital. Because of my nan, I’ve always had a personal interest in how we use prosthetics in the heart.
Prior to the surgery, my nan was given the choice between mechanical or biological valves, each with their own pros and cons. Biological valves typically last 10-15 years while mechanical valves can last a lifetime, making mechanical the go-to for patients under 65. Her team opted for mechanical valves so she wouldn’t need yet another risky open-heart surgery later down the line. 1
Figure 1: Diagram of the heart valves, alongside biological and mechanical valve replacements.2
Biological 0 – Mechanical 1
Figure 2: Video showing how mechanical valves work.3
Despite this clear win for mechanical valves, they come with a major drawback – being prone to causing blood clots, which could lead to heart attacks or strokes. As such, patients with mechanical heart valves must take anticoagulants for the rest of their lives.
For my nan, this meant she had to take warfarin and required blood testing (by INR) every week to maintain the right ‘thickness’ of blood – too thick and you risk blood clots, too thin and you risk uncontrollable bleeding.4
Biological 1 – Mechanical 1
Biological valves not needing anticoagulation is an obvious score, however, there’s issues with xenotransplantation to consider. The majority of valves come from pigs or cows, meaning concerns are raised for animal welfare. To ensure the animal is healthy enough to provide a ‘safe’ transplant, they must be kept in sterile and confined laboratory conditions. In some ways this may be better than the conditions livestock have, but it’s still lacking for the animal’s nature. Having ‘good ethics’ is absolutely a requirement here.5
Figure 3: Video showing how a biological valve works. 6
These are only a few of the positives and negatives for each traditional type of heart valve. It’s a complex decision and will depend entirely on the patient. However, in the time since my nan got her valves replaced, science and medicine has advanced. Open-heart surgery is still the norm for valve replacement, but transcatheter aortic valve implantation (TAVI) can now be used to avoid the obvious risks of open-heart surgery.
Another development is tissue engineered heart valves. This involves taking a scaffold which is seeded with stem cells and then then grown in a bioreactor before implantation. This would avoid the hazards associated with anticoagulation for mechanical valves, and the ethical issues of animal biological valves – and could grow along with the development in paediatric patients. Tissue engineered valves have not yet reached the clinical trials stage, but research is developing every day.8
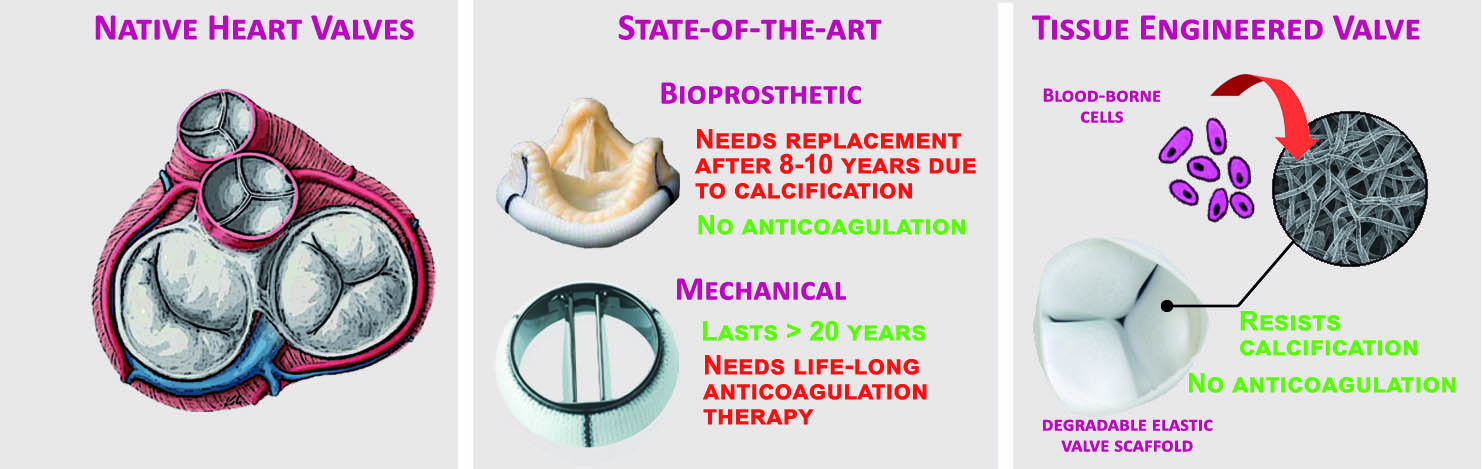
Figure 5: Comparison between native, biological, mechanical and tissue engineered heart valves9
With the heart being such an important organ, any improvements to the current procedures for replacement heart valve prosthetics are hugely beneficial. I’ve loved finding out more about how research is advancing in an ever-present field in mine and my family’s lives. One day I might be telling the future generations about how scientists grew new heart valves in a lab for me!
Mendelson, K. & Schoen, F. J. Heart valve tissue engineering: concepts, approaches, progress, and challenges. Ann Biomed Eng34, 1799-1819 (2006). https://doi.org/10.1007/s10439-006-9163-z↩︎
Copy. Delete. Paste. Three words we all subconsciously think as we comb through text during our daily lives. Three words that I’ve been repeating endlessly as I spend countless hours cutting and pasting lines of code, desperately trying to make my third-year university project work. Combining the realisation of what an invaluable yet simple tool we have everyday access to and my studies in Biomedical Engineering, I began wondering if we could apply a similar gadget to our own DNA, removing any sequences we deem “undesirable” and replacing them with something of our choosing.
This led me to the discovery of Clustered Regularly Interspaced Short Palindromic Repeats, also known as CRISPR, which allows us to do exactly that, opening up a world of opportunities to cure disease as well as further the abilities of other biotechnologies – you can read more about the potential of a fascinating combination of stem cells and CRISPR-Cas9 here!
How does it work?
See below a brief video which explains how CRISPR-Cas9 is capable of editing our DNA!
Transcript: In a document, if we suspect we’ve misspelled a word we can use the find function to highlight the error and correct it or delete it. Within our DNA that function is taken on by a system called CRISPR/Cas9. CRISPR is short for clustered regularly interspaced short palindromic repeats. CRISPR consists of two components – the Cas9 protein that can cut DNA and a guide RNA that can recognise the sequence of DNA to be edited. To use CRISPR/Cas9, scientists first identify the sequence of the human genome that’s causing a health problem. Then they create a specific guide RNA to recognise that particular stretch of a’s, t’s, g’s and c’s in the DNA. The guide RNA is attached to the DNA cutting enzyme Cas9 and then this complex is introduced to the target cells. It locates the target letter sequence and cuts the DNA at that point. Scientists can then edit the existing genome by either modifying, deleting or inserting new sequences, effectively making CRISPR/Cas9 a cut-and-paste tool for DNA editing. In the future, scientists hope to use CRISPR/Cas9 to develop critical advances in patient care or even cure lifelong inherited diseases.
How could it be used?
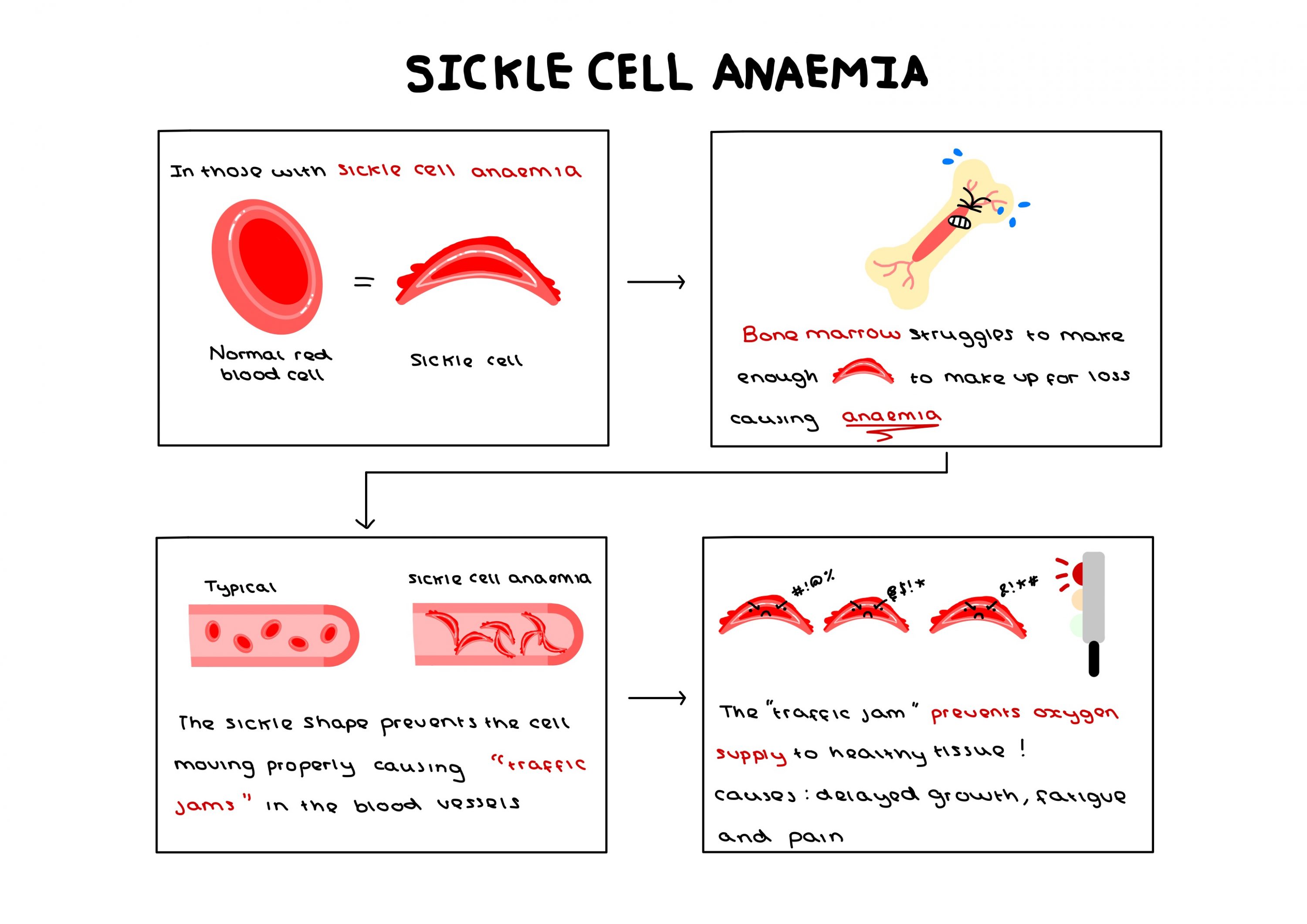
One potential application of CRISPR-Cas9 currently being investigated surrounds sickle cell anaemia, an incurable genetic disease with only expensive and harmful treatments available. The potential to undergo a singular procedure to completely cure this condition is revolutionary – a potential that could be applied to up to 8,000 more genetic mutations.
However, the capacity for this technology is so great that I find myself beginning to fear what it could be used to eradicate instead of simply treat. Concerns are already being raised by scholars with genetic differences, statements such as “our genetic conditions are not simply entities that can be clipped away from us as if they were some kind of a misspelled word or an awkward sentence in a document” being published in scientific news journals, highlighting that someone is still human despite their differences. The desire to completely remove a gene from society assumes that people with such genes are constantly suffering, their gene pool contaminated and inherently inferior.
Personally, I carry the genetic mutation for haemochromatosis, a condition that means I will most likely be subject to regular venesection in my later adult years. Whilst I have no affinity for my condition, viewing it as separate to myself and something that I would readily “delete”, having access to the support groups has shown me how it can bring people together and create a beautiful community – something that can make some feel positively connected to their condition. The idea that we could use CRISPR-Cas9 to not only treat genetic diseases but instead completely remove them from existence raises the question of whether this technology is a cure or a threat to these communities.
Ethical Parallels
A parallel can easily be drawn between the ethical issues surrounding the application of CRISPR-Cas9 in curing instead of treating genetic diseases and those restricting gene editing on embryos. As of March 2025, it is illegal to perform gene editing on embryos for reproduction in the UK, “designer babies” being labelled as a “ethical horrors waiting to happen” by news companies as profound as The Guardian.
As a society we must be careful as we toe the line between providing the best quality of life and removing people’s individuality, a line that could easily be crossed by both of these technologies. In the end, I struggle to distinguish the difference between editing an embryo’s genes to create what is considered an “ideal” baby, a process that is currently illegal, and “perfecting” the genes that somebody already lives with. Despite this, I also wonder whether it is truly ethical to leave somebody wishing for a cure when one is sat right within our reach.
But in the end, how would you feel if a fundamental part of what made you you could be so easily erased from existence?
When we first looked at gene editing, I had mixed feelings. As some who studies engineering, I believe in innovation and using technology to help people. However, as some whose sibling has a disability, I thought about how the advancement of gene editing pushes the narrative that those with disabilities need ‘fixing’. Therefore, I decided to research the topic further.
First of all, what is gene editing?
Gene editing is the process of deleting, inserting or replacing genetic material within animals, plants and bacteria to alter their characteristics. It has different applications, but I’m focusing on gene therapy and using different techniques to treat diseases. The development of CRISPR-Cas9 has created a quicker, cheaper method for gene editing, leading to the current buzz around the topic.
Laws surrounding gene editing:
While it is illegal in the UK to implant a gene-edited embryo, in 2016, the HFEA approved licensing to allow gene editing of human embryos in research. Many of my classmates thought this was a good change as it could lead to more knowledge and potential cures about inheritable disorders like Cystic Fibrosis. However, is this any different from previous attempts in eugenics? The removal of genetics at an embryonic level will lead to the eradication of different, ‘undesirable’, traits from society. The practice may also lead to the relaxation of laws and the possibility of designer babies.
Gene therapy case:
While gene editing is often associated with inheritable disorders, it can be used to cure cancer. There have been successful results from a study in 2010, where a patient suffering from lymphoma underwent CAR T cell therapy. In this treatment, the patients T cells are collected and then genetically altered in the laboratory so they can recognise the cancerous cells. They are then put back inside the body to fight the cancerous cells.
However, gene therapies are expensive! In the US it is estimated that $20.4 billion is spent annually on gene therapies. If this money was spent on creating a more inclusive environment through education of the public and the changing of laws, this could have a far greater effect on the people already living with genetic disorders. Is it not better to create an environment where people can live well with these disorders, then create one which focuses on their removal?
Different opinions:
The NHGRI conducted surveys to investigate patient perspectives on gene editing. Many patients, especially those with Huntington’s, argued that gene editing should be used to prevent other people from inheriting the disease, despite the argument that it could isolate them from society and reinforce the belief that people with disabilities have a low quality of life.
Furthermore, Wellcome Connecting Science hosted a citizen’s jury vote based on the following question: ‘Are there any circumstances under which a UK Government should consider changing the law to allow intentional genome editing of human embryos for serious genetic conditions?’. All the jurors had been affected in one way or another by hereditary diseases and by the end most jurors (17-4) agreed that human embryos should be edited. While a small sample, this vote indicates that the scientific community and the legislators are listening to those who it truly affects, something which has previously been overlooked and distinguishes gene editing from previous, eugenic practices.
Final Thoughts
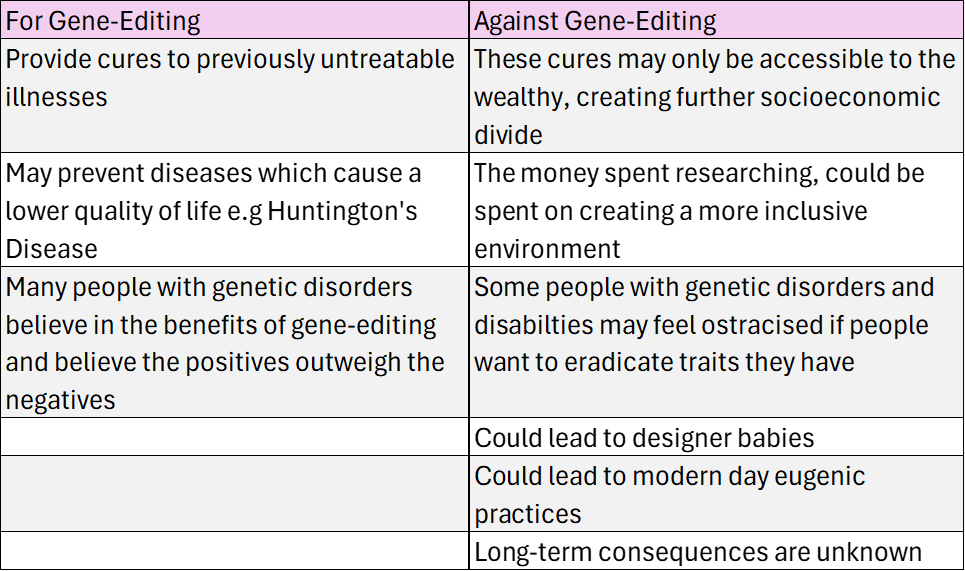
My summary of different arguments for and against Gene-Editing
I believe that the advancement of gene editing will help those with genetic disorders and provides cures which were previously unavailable. I think that this outweighs the negatives of gene editing especially considering many people with genetic disorders believe in the benefits. However, I think that the narrative surrounding gene editing needs to include those who are affected the most to make sure that it is continuing to be done in a positive way which doesn’t isolate people or become modern-day eugenics.
Several cases of end-stage organ failure have been treated successfully through organ transplantation. An organ transplant is performed if a specific organ is about to fail and must be replaced to maintain its functioning [1]. The NHS states that 8006 individuals are waiting to receive a transplant in the UK, and 3409 individuals have received one [2]. The demand is more than the supply of organs. Artificial organs are an engineering wonder that can be used to replace organ transplantation.
What are Artificial Organs?
Artificial organs are devices manufactured by humans that substitute failing organs. The devices are made synthetically or using a blend of synthetic material and living cells. Bioengineered tissues like liver scaffolds and artificial skin are typical examples, as are artificial hearts, kidneys, and lungs. Artificial Organs have the ability to address much of the problem involved in the study of organ transplantation
3-D bioprinting artificial organs[4]
Artificial organ heart [3]
Advantages of Artificial Organs
One of the major challenges is a lack of donor organs. Artificial organs remove the issue of reliance on human donors. This helps in the decrease in waiting lists and organ shortage. Occasionally, there is a possibility of organ rejection; to avert this, transplants need immunosuppressive medications, which can cause infections or cancer. The likelihood of this is ruled out or diminished by artificial organs produced from the cells of the patient themselves. Organ transplantation has a limited shelf life and needs to be transplanted soon. But artificially produced organs can be preserved until required and thus can be manufactured in bulk. Moreover, human donor organs come with ethical issues of consent and organ trafficking. Artificial organs present a solution to this dilemma, minimizing the ethical issues regarding human donors.
Disadvantages of Artificial Organs
Artificial organs are highly expensive because of the numerous complications involved in mimicking the intricate functions of natural organs while producing them that renders them unaffordable for most individuals. Even though it reduces the risk of infections caused due to immunosuppressive drugs, artificial organs require continuous monitoring and maintenance to make sure they are working at full efficiency. Replication of intricate organs like the liver and kidneys is still in research. Similar to organ transplantation, artificial organs also present ethical and regulatory challenges. There must be a balance between patient safety and experimental progress. Hence testing artificial organs involves a long approval process for clinical applications.
Conclusion
Artificial organs are the future of organ transplantation and a possible cure for the organ shortage crisis. Nevertheless, there are various challenges that have to be overcome, including cost, technical challenges and ethical legislation. Organ transplantation cannot yet completely be replaced with artificial organs but they do hold promise for an era when life-saving treatments will be more universally available and feasible.
References
[1] Saidi, R.F. and S K Hejazii Kenari (2014). Challenges of Organ Shortage for Transplantation: Solutions and Opportunities. International Journal of Organ Transplantation Medicine, [online] 5(3), p.87. Available at: https://pmc.ncbi.nlm.nih.gov/articles/PMC4149736/.
[2] NHS (2023). Statistics about organ donation. [online] NHS Organ Donation. Available at: https://www.organdonation.nhs.uk/helping-you-to-decide/about-organ-donation/statistics-about-organ-donation/.
[3]https://www.biospace.com/mark-terry (2018). Artificial Organs for Biopharma Research and More. [online] BioSpace. Available at: https://www.biospace.com/artificial-organs-for-biopharma-research-and-more.
[4] Wood, I. (2023). 3D bioprinting artificial organs could become quicker and easier. [online] Drug Target Review. Available at: https://www.drugtargetreview.com/news/110266/3d-bioprinting-artificial-organs-could-become-quicker-and-easier/.
Following the Sensor Lectures given by David Simpson and Russel Torah, the idea of optical imaging really stood out to me. Additionally, my passion for neuroscience and the brain brought me to cerebral optical imaging. Upon initial research, I noticed the most documented imaging techniques included MRI, CT and PET scans. PET scans, or positron emission tomography involves the use of a radio tracer that emits positively charged particles. When these particles encounter an electron, they completely annihilate and generate two gamma rays that can be picked up by the PET scanner. I had known about annihilation from physics at school, but I never knew to could be used to image the body! Since the radiotracer gets absorbed into more active tissues. This makes PET unique as it’s a way to image the functionality of tissues.
Looking closer into functional imaging, I came across functional MRI (fMRI) and fNIRs. While fMRI builds on current MRI technology, it involves the patient to stay still while completing tasks. While I knew this was still useful, I found that fNIRs could be used while moving around, so that, in my opinion it was much more potential in comparison.
fNIRs: A Quick Rundown
Functional near infrared spectroscopy, is a functional cerebral imaging method. It involves the use of near infrared light, between 700-950nm wavelengths. This is because once you get to the near infrared, the body is nearly transparent! Using a source, like an LED you pass the light through the body where the light follows a banana shape towards a detector just next to the source. I found this particularly strange, it made me think how light of all wavelengths of light pass through the body.
This is a short video on the underlying principles of fNIRs.
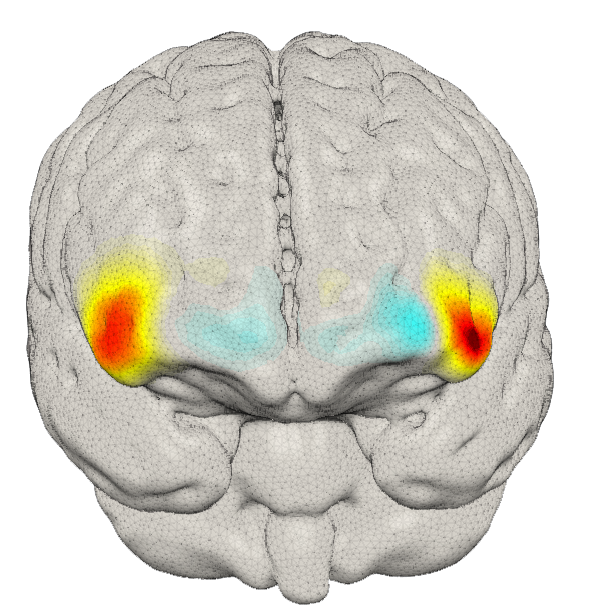
You may have noticed there aren’t any images being generated by fNIRs. This is because in order to generate images you must use Diffuse Optical Tomography (DOT). Simply put, DOT involves using lots of fNIRs sources and detectors and overlapping them to generate an image. Using these images in conjunction with a functional experiment, you can see which areas of the brain ‘light up’ when conducting particular activities. Since fNIRs can be used while moving, the sky is the limit when coming up with experiments to conduct.
The Promising Future of fNIRs/ Reflection
After discovering this promising technology, I felt compelled to write about it. I found its resistance to motion artifacts particularly interesting, as a biomedical engineer, they are something I have to deal with in all of my projects. Additionally, this feature means fNIRs has the potential to investigate infant brains as MRI and fMRI require the patient to stay very still, which can be very difficult for infants and children.
A researcher at the University of Southampton; Dr Ernesto Elias Vidal Rosas, is currently working on an fNIRs system that will tackle the issue of the lower spatial resolution, one of the main drawbacks of the technology. He inspired me to investigate this technology after discovering one of his written papers on the topic.
Personally I see this technology rivalling that of fMRI in its researching capabilities in infants not only due to the motion resistance but also the ability to conduct naturalistic experiments, potentially using technology like VR in order to investigate the brain’s activity when interacting with the world outside the lab. Additionally, the sensor could be used in other areas of the body for example, when placed just below the ribcage, “[fNIRs] has shown promise in being a more accurate, and less bias sensor compared to the gold standard”, Dr Ernesto Elias Vidal Rosas.
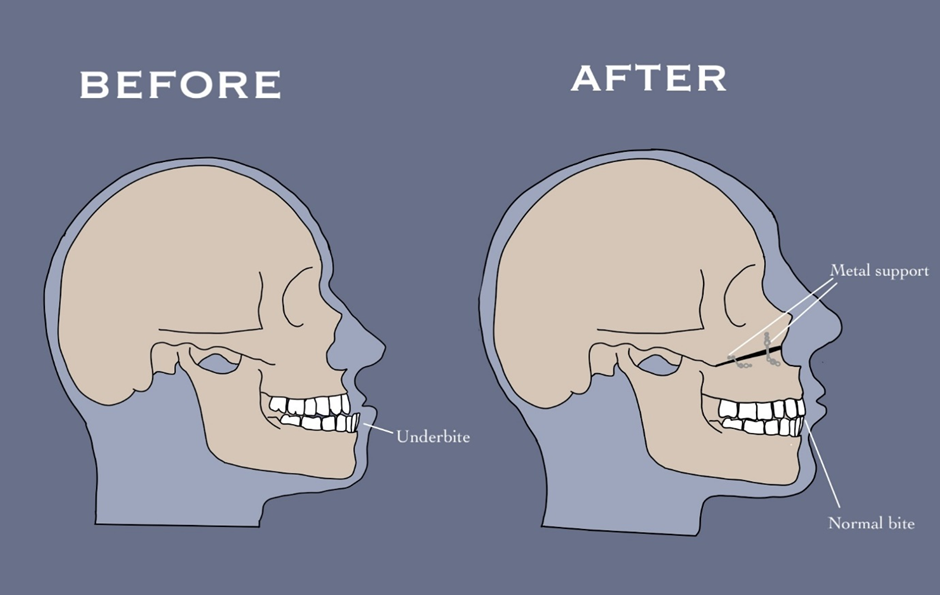
After learning about prosthesis (replacing a body part or joint) and orthosis (external support promoting healing) I reflected on my own experience. I had a Le Fort I osteotomy, a surgery to reposition the upper jaw. This doesn’t fit either prosthetic or orthosis categories, but is somewhere in between. I knew metal implants were used for this, but hadn’t considered why or how they work.
The best person to learn from was the surgeon himself, so on my previous visit I interviewed with questions based on topics discussed in the lecture:
Me: What material was used in the metal implants and why?
Surgeon: Medical grade titanium, because its biocompatible
Me: How was the metal implanted to hold the jaw?
Surgeon: There are two stages. Primary stability is done in surgery, it’s the tightening of screws into the bone and then you find the bone grows in the threads of the screws and will grow in and over and around the plates, osteointegration it’s called and that’s the secondary stability
Me: How does it change for different sizes and shaped jaws?
Surgeon: There’s a website here, you can even find the whole guide if you want about all the screws they make and where they use them, different plates, different sizes. So, in the face depending on how much load it has to take you change how thick the plates are.
The website mentioned, which allowed me to visualise how the implants were used:
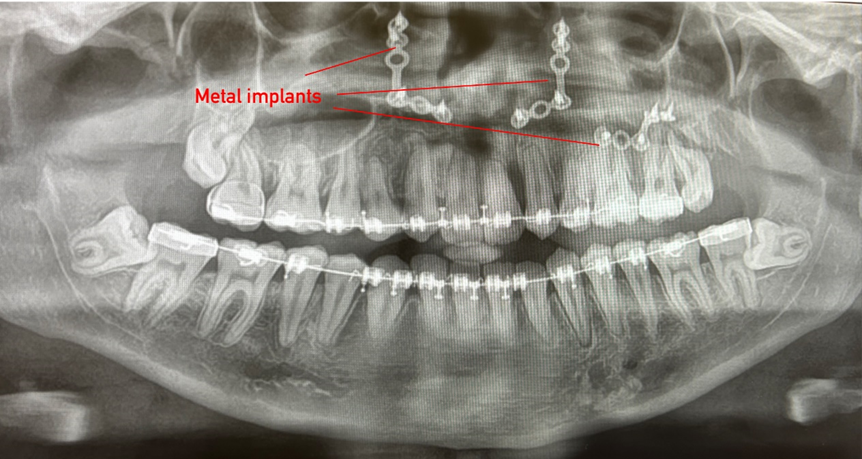
He provided me with my x-ray, showing exactly how the implants are positioned:
The interview, the website and x-ray gave me a deeper understanding of the role of the metal implants. This led me to create this image, showing how the implants are used:
The interview revealed similarities between facial implants and joint replacements, particularly the porous material that I observed in the practical, which allows bone to grow into to stabilise.
Although biomedical engineers design implants to reduce failures, they do occur due to infection, breakdown between implant and bone, and migration of implant. The lecture on this topic made me curious if the same was true for metal implants in the face.
Further reading showed in a study of 485 orthognathic cases, 93 complications were recorded, including failure of fixation, requiring re-intervention (Zaroni et al. 2019). This made me reflect on the ethical considerations when offering this surgery. Unlike prosthetics, which are needed due to pain, orthognathic surgery, is often for aesthetics and ease of eating, both of which are not essential. This raises an ethical dilemma: if not needed, is it worth the risks, even if minimal?
The legal and ethical solution to this is informed consent. This video helped me understand what this actually entails:
I felt the NHS definitely achieved this in my case by repeated discussions over several years. However, I believe knowing the risks doesn’t compare to experiencing them. Something I found extremely useful before my surgery was finding others on social media who had had the same or similar procedures. It showed me the reality of recovery and possible complications. I believe informed consent could be improved by sharing first-hand experiences so I designed a template for a website which would facilitate this.
This would allow more in-depth discussions on what the recovery process is like and how other people experienced complications, rather than just the surgeons’ perceptions. Personally, the minimal risks were worth the outcome, but seeing others who had same procedure helped me make a truly informed decision.



![[9] An image showing the structure of a microbubble responding to ultrasound waves produced by a Transducer during ultrasound scanning in Pregnancy](https://generic.wordpress.soton.ac.uk/uosm2031-2025/wp-content/uploads/sites/529/2025/03/image-64.png)






This is a good blog. It nicely demonstrates a good understanding of organ-on-a-chip technology and clearly explains its purpose and…
This is a good blog, very engaging with a good backgroud to 3D bioprinting. You could improve your blog with…
This is a good, very interesting blog about necrobotics. It explores the idea of necrobiotics which is fairly new approach…
This is a good blog. You introduce the reader to the topic of prosthetics and bionic limbs in a very…
This is a good blog introducing hernia mesh benefits and drawbacks. You create a narrative in this blog, which showcase…