3.8 Vulnerability data
Vulnerability to ill health can be thought of as a combination of pre-disposing factors and behaviour. Pre-disposing factors might include age, sex or ethnicity. For example, melanoma (skin cancer) is more common among those of European origin and this is an inherited genetically increased risk not related to any behaviour. Behaviour also affects the risk of ill health. For example, consuming a diet of energy-dense foods leads to an increased risk of cardiovascular disease, diabetes and hypertension.
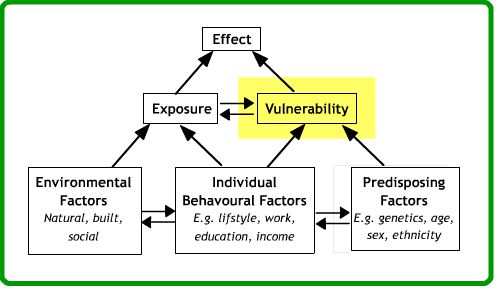
It should be borne in mind that whilst vulnerability directly relates to behaviour and predisposing factors, there are more subtle links to other parts of the diagram above. Behaviour is clearly affected by environmental conditions. For instance, obesity is associated with a behavioural risk of eating energy-rich foods, yet in some neighbourhoods (so-called ‘food deserts’) fresh fruit and vegetables may be difficult to obtain. Similarly, washing of hands is very difficult for those without a mains water supply or the means to buy soap. Behaviour and predisposing factors themselves are also closely related. Infection rates for many sexually transmitted diseases peak among the 20-40 year age group. There is no particular physiological reason why people in this age group are more at risk and so age in this context acts as a proxy measure for risky behaviour. Thus, environment may affect behaviour and predisposing factors and behaviour are also inter-related.
It is comparatively easy to obtain data on age, sex, and ethnicity and measure these variables. Age and sex are included in all census data and most health survey data. Most respondents can remember their age and have little reason to provide false information on these variables.
In contrast, behavioural data are much harder to obtain. Other than occupation, which is recorded in most censuses, observations about behaviour are often self-reported in sample surveys that cover only a small proportion of the study population. Data on behaviour for all of the population living in a given area is usually either very limited or non-existent. However, very occasionally, information on behaviour can be obtained by cross-referencing data sets, such as health records with car ownership records. In sample surveys, questionnaires are sometimes used to obtain information about behaviour, but responses to such questions are notoriously unreliable. For example, sexual behaviour is often the focus of social stigma and answers to questions about numbers of sexual partners may prove unreliable as a consequence. Similarly, in developing countries, many households are aware that hand-washing reduces diarrhoeal disease and so may claim in interview to wash their hands regularly when this is not the case. Asking to be shown the household’s bar of soap may provide a better measure of hygiene behaviour than direct questions about hand-washing in such developing country settings.
Activity
Coronary heart disease (CHD) is a health complaint that occurs when the coronary arteries become narrowed or clogged and cannot supply enough blood to the heart. Read the references below relating to CHD, then answer the following questions:
-
- Are there any predisposing factors that may increase the risk of suffering coronary heart disease? If so, who is at risk?
Answer 1
Men are widely regarded as being more susceptible to CHD than women. Furthermore, the risk of CHD increases with age. Ethnicity also influences risk with those of Afro-Caribbean origin being at greater risk of coronary heart disease than the population as a whole. Similarly, a family history of heart disease is associated with greater risk of heart disease too.
Hide
-
- Are there any behavioural factors that may enhance the risk of CHD?
Answer 2
One of the most obvious behaviours that is associated with coronary heart disease is smoking. Excessive drinking also increases the risk of heart disease, although moderate drinking does not. Another CHD risk factor related to behaviour is lack of exercise and physical inactivity.
Hide
Ultimately, many GIS-based analyses of disease causality are used to plan interventions that reduce disease rates. Do you foresee any problems with intervention measures that target behaviour (for example, banning smoking in restaurants / bars or making nicotine patches at low cost)?
Activity
Download the zip file and complete the practical described in the .pdf file, which involves estimating CHD cases for general practices in the Cardiff area of the UK. It uses a simple version of a technique called areal interpolation and instructions are available in the zip for both ArcGIS Desktop and Pro.
References (Essential reading for this learning object indicated by *)
* The World Heart Federation provides an overview of the risk factors associated with coronary heart disease: http://www.world-heart-federation.org/cardiovascular-health/cardiovascular-disease-risk-factors/
Martin, D., and Wright, J. (2009) Disease prevalence in the English population: a comparison of primary care registers and prevalence models. Social Science and Medicine 68 (2), 266-74.
This exercise is loosely based around the reference above, but note you do not have to read the reference in order to complete the exercise.